
Pneumonia is a frightening word. If you imagine your lungs as an upside-down tree, the leaves are millions of tiny air sacs called alveoli. When you are healthy, these sacs fill with air and pass oxygen into your blood. When you have pneumonia, these tiny sacs become inflamed and fill with fluid or pus. This makes it incredibly hard to breathe.
For decades, doctors have treated pneumonia caused by common bacteria and seasonal viruses. However, when the SARS-CoV-2 virus emerged, doctors noticed something unusual. The pneumonia caused by COVID-19 did not look or behave like the pneumonia they were used to seeing. Patients required breathing machines more often, their blood clotted in strange ways, and their hospital stays stretched on for weeks.
This raised a core question in the medical community. Is COVID-19 pneumonia fundamentally worse than regular pneumonia, or is it just different?
By comparing how COVID-19 and other illnesses attack the lungs, scientists have uncovered important clues about how our immune system works, who is most at risk, and how we can better protect ourselves.
How COVID-19 Pneumonia Actually Works
To understand why COVID-19 pneumonia is unique, we have to look at how the virus enters the body. The SARS-CoV-2 virus has spike proteins on its surface. These spikes act like keys that unlock specific doors on our cells called ACE2 receptors.
These receptors are found in high numbers in the lungs. When the virus enters the lung cells, it begins to multiply. But the virus itself is only half of the problem. The other half is how your body responds to the invasion.
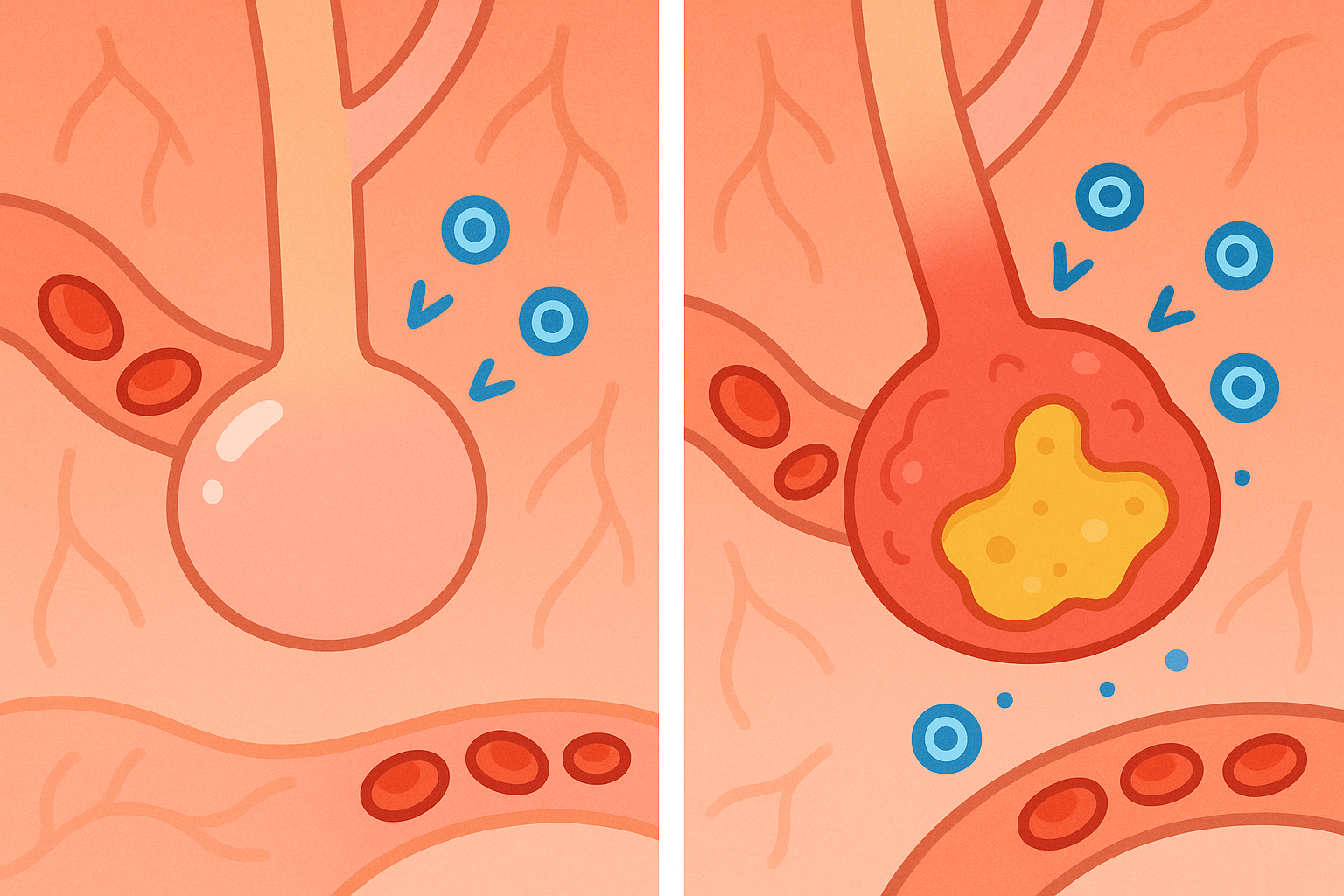
When the immune system detects the virus, it releases chemical messengers to call for backup. These messengers are called cytokines (SIGH-toe-kines). In a healthy response, cytokines help fight off the infection and then fade away.
In severe cases of COVID-19, the immune system panics. It releases too many of these messengers, creating a massive inflammatory response known as a cytokine storm.
A 2020 review in the Journal of Autoimmunity explains that this storm triggers a condition called Macrophage activation syndrome (MAK-roh-fahj ak-tuh-VAY-shun SIN-drome). This happens when white blood cells, which usually eat dead cells and bacteria, go into overdrive and start damaging healthy lung tissue. This extreme inflammation is what causes the lungs to fill with fluid so rapidly in severe COVID-19 cases.
What the Research Shows: COVID-19 vs. Traditional Pneumonia
To figure out exactly how COVID-19 pneumonia compares to traditional pneumonia, researchers had to look at patients side-by-side.
A 2021 study in the Annals of Medicine compared 53 patients with COVID-19 pneumonia to 50 patients with non-COVID-19 pneumonia. All patients were admitted to the same hospital during the early months of the pandemic.
The findings highlighted some surprising differences:
- Age and General Health: The patients with traditional pneumonia were generally older (average age 72) and had more existing health problems, like chronic kidney disease and neurological issues. The COVID-19 patients were younger (average age 61) and generally healthier before getting sick.
- Breathing Support: Even though the COVID-19 patients were younger, they required non-invasive ventilation (breathing machines) much more often than the traditional pneumonia group (19% versus 2%).
- Length of Stay: The most striking difference was how long it took to recover. Patients with traditional pneumonia stayed in the hospital for an average of 9 days. Patients with COVID-19 pneumonia stayed for an average of 30 days.
Despite these differences, the overall in-hospital mortality rate was actually slightly higher for the traditional pneumonia group (24%) compared to the COVID-19 group (17%), though researchers noted this difference was not statistically significant. The high death rate in the non-COVID group was likely because those patients were older and frailer to begin with. Related: What Science Actually Says About Frailty in Older Adults
Comparison: COVID-19 Pneumonia vs. Non-COVID Pneumonia
| Measurement | COVID-19 Pneumonia | Non-COVID Pneumonia |
|---|---|---|
| Average Age | 61.5 years | 72.7 years |
| Needed Breathing Machine | 19% | 2% |
| Average Hospital Stay | 30 days | 9 days |
| In-Hospital Mortality | 17% | 24% |
The Hidden Risk: Blood Clots and Vascular Damage
One of the most dangerous differences between COVID-19 and traditional pneumonia is what happens outside the lungs. The ACE2 receptors that the virus targets are not just in the lungs. They also line our blood vessels.
When the virus attacks the blood vessels, it causes widespread inflammation. This makes the blood thicker and more likely to clot.
A 2022 study in the Journal of Stroke and Cerebrovascular Diseases examined 368 patients hospitalized with COVID-19. They found that 13.3% of these patients suffered an ischemic stroke, which happens when a blood clot blocks blood flow to the brain. The researchers noted that patients with certain heart characteristics, like an enlarged left atrium, were at an even higher risk for these clots.
These clots do not just affect the brain and lungs. They can happen anywhere. A 2023 review in Graefe’s Archive for Clinical and Experimental Ophthalmology found that COVID-19 can even cause blood clots in the eyes. Researchers documented multiple cases of retinal artery occlusions (eye strokes) and retinal vein occlusions in COVID-19 patients. These blockages can lead to sudden vision loss, proving that the virus is truly a full-body disease, not just a lung infection.
Who Needs Extra Caution
While anyone can develop severe COVID-19 pneumonia, certain underlying conditions make the risk much higher.
People with Cancer: Because cancer treatments often weaken the immune system, doctors were initially very concerned about cancer patients catching COVID-19. A 2021 study in Future Oncology looked at 260 hospitalized COVID-19 patients, 57 of whom had cancer. Surprisingly, the mortality rate was not significantly different between the cancer and non-cancer groups. However, the cancer patients did require longer hospital stays. The researchers found that obesity and active smoking were actually much stronger predictors of death than a cancer diagnosis.
People with HIV: A 2023 study in The Journal of Infectious Diseases looked at population data in New York City. Researchers found that people living with HIV had a 30% higher risk of both hospitalization and death from COVID-19 compared to people without HIV. This risk was especially high for those with low CD4 white blood cell counts, emphasizing the need for careful monitoring in this population.
How Vaccines Change the Picture
Vaccines have drastically changed the landscape of COVID-19 pneumonia. They work by training the immune system to recognize the virus’s spike protein before an actual infection occurs.
A 2021 study in The New England Journal of Medicine tracked nearly 4,000 frontline workers. The researchers found that mRNA vaccines were highly effective at preventing infection. Even more importantly, when vaccinated people did get sick (breakthrough infections), their viral load was 40% lower than unvaccinated people. They also spent fewer days sick in bed and had a 58% lower risk of developing a fever.
However, the protection vaccines offer against spreading the virus does decrease over time. Another study in The New England Journal of Medicine found that while vaccines reduce the onward transmission of the virus, this protective effect wanes after a few months, especially with newer variants like Delta. This is why booster shots and updated vaccines remain an important part of public health strategy.
Where The Science Is Still Uncertain: Life After the Hospital
Surviving severe COVID-19 pneumonia is a major victory, but leaving the hospital is often just the beginning of the journey. Scientists are still studying how long it takes for the lungs to fully heal.
A 2021 study in The Lancet followed 1,733 patients for six months after they were discharged from a hospital in Wuhan, China. At the six-month mark, 63% of patients still reported fatigue or muscle weakness.
More concerning was the state of their lungs. Among the patients who had the most severe pneumonia during their hospital stay, 56% still had diffusion impairment six months later. This means their lungs were still struggling to efficiently transfer oxygen into their bloodstream. Researchers are continuing to track these patients to see if this lung damage is permanent or if it slowly improves over years. Related: What Science Actually Says About Long COVID Symptoms and Treatment
Common Questions About COVID-19 Pneumonia
Can you tell the difference between COVID-19 pneumonia and regular pneumonia from an X-ray?
Yes, often. COVID-19 pneumonia typically affects both lungs and creates a “ground-glass” appearance on a CT scan or X-ray. Bacterial pneumonia often affects just one specific lobe or section of the lung.
Why do some people get COVID-19 pneumonia and others just get a cold?
It depends on a mix of factors, including age, underlying health conditions, how much virus you were exposed to, and your specific immune system. A hyperactive immune response (cytokine storm) is a major reason why the infection moves deep into the lungs for some people.
Does COVID-19 pneumonia cause permanent lung damage?
In many cases, the lungs heal completely. However, severe cases can lead to scarring (pulmonary fibrosis), which can cause long-term breathing difficulties.
The Bottom Line / Takeaways
- COVID-19 pneumonia behaves differently than traditional pneumonia. It is characterized by severe, widespread inflammation and a hyperactive immune response called a cytokine storm.
- While traditional pneumonia heavily impacts older, frailer adults, COVID-19 can cause severe lung failure in younger patients, leading to much longer hospital stays and higher rates of mechanical ventilation.
- The SARS-CoV-2 virus also attacks blood vessels, making blood clots, strokes, and even eye blockages a serious risk during severe infections.
- Underlying conditions like obesity and smoking are massive risk factors for severe outcomes, sometimes even more so than a cancer diagnosis.
- Vaccines significantly reduce the amount of virus in the body and shorten the duration of the illness, protecting the lungs from severe damage.
- Recovery can be slow. Many patients who survive severe COVID-19 pneumonia still struggle with fatigue and reduced lung capacity six months later.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| COVID vs. Non-COVID Pneumonia | COVID-19 patients required much longer hospital stays (30 days vs 9 days) and more ventilation, though mortality rates were statistically similar in this cohort. | PMID 34854790 |
| Long-Term Lung Recovery | Six months after hospitalization, 56% of severe COVID-19 patients still had impaired oxygen transfer in their lungs. | PMID 33428867 |
| Vaccine Effectiveness | mRNA vaccines reduced viral load by 40% and shortened illness duration in breakthrough infections. | PMID 34192428 |
| Stroke Risk in COVID-19 | 13.3% of hospitalized COVID-19 patients in the study suffered an ischemic stroke, driven by blood vessel inflammation. | PMID 34826678 |
| Cancer and COVID-19 | Obesity and smoking were stronger predictors of mortality than a cancer diagnosis, though cancer patients had longer hospital stays. | PMID 34263660 |
| Autoimmunity and COVID-19 | The virus can trigger a “cytokine storm,” leading the immune system to attack healthy lung tissue and blood vessels. | PMID 32563547 |
Last updated: March 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.


Leave a Reply