If you have ever experienced the sharp, shooting pain of a pinched nerve in your back or neck, you know how debilitating it can be. This pain, often called sciatica when it shoots down the leg, is most commonly caused by a herniated disc.
When faced with this intense pain, many people assume that surgery is the only way to fix the problem. However, modern research paints a very different picture. Science shows that the body has a remarkable ability to heal herniated discs on its own, and when medical intervention is needed, the best approach depends heavily on timing, symptoms, and the specific location of the injury.
This article breaks down what peer-reviewed research reveals about how herniated discs heal, how conservative treatments compare to surgery, and what to expect if you do need an operation.
How This Might Work: The Anatomy of a Herniated Disc
To understand how treatments work, it helps to understand what a spinal disc actually is. The discs between your spinal bones act as shock absorbers. You can think of them like jelly donuts.
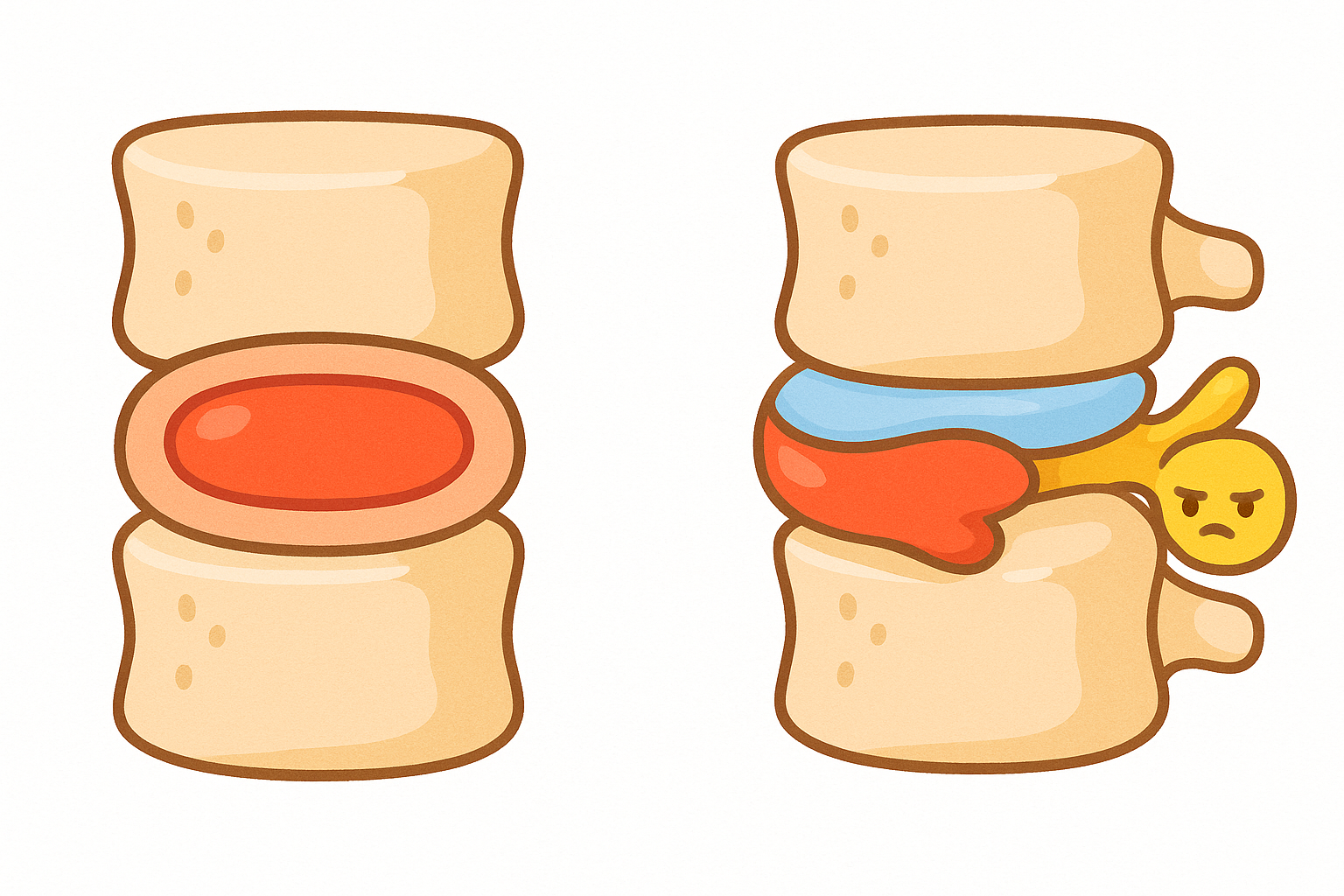
They have a tough, flexible outer ring called the annulus fibrosus (AN-yoo-lus fy-BROH-sus) and a soft, gel-like center called the nucleus pulposus (NOO-klee-us pul-POH-sus).
When the outer ring tears due to wear and tear, injury, or sudden pressure, the inner gel can squeeze out. This is a herniated disc. The extruded gel can press against nearby spinal nerves. Furthermore, the gel contains inflammatory chemicals that irritate the nerve, causing pain, numbness, or weakness to radiate down the arm or leg.
Related: Treating Neuropathic Pain: What the Latest Science Says
What the Research Shows
The Healing Power of Time
Perhaps the most comforting finding in spinal research is that a herniated disc is usually not a permanent condition.
A broad review of lumbar disc herniation in Neurocirugia found that the natural history of the condition is highly favorable. In fact, for the vast majority of patients, the pain resolves or improves substantially within four to six weeks.
How does this happen? When the disc material herniates into the spinal canal, your immune system recognizes it as a foreign invader. White blood cells called macrophages attack and break down the extruded gel, gradually shrinking the herniation and relieving pressure on the nerve.

Conservative Treatment: Therapy and Medication
Because the body can often heal itself, doctors typically recommend starting with conservative care. This includes rest, physical therapy, and pain management.
Targeted exercises can help relieve pressure on the affected nerves. A 2022 study in BMC Musculoskeletal Disorders observed patients with cervical (neck) disc herniations undergoing an 8-week therapeutic exercise program. Using video imaging, researchers found that specific active movements, like retracting the neck or flexing away from the painful side, physically increased the space around the spinal nerves, leading to significant symptom relief.
When exercise and time are not enough to manage the pain, medications are often used. However, the evidence for some medications is mixed. A systematic review in Orthopadie looked at the use of systemic steroids (like oral prednisone) for neck pain caused by pinched nerves. The researchers found very limited evidence overall, though one high-quality trial did show that oral steroids provided better pain relief and functional improvement than a placebo. Epidural steroid injections, which deliver medication directly to the spine, are also commonly used and show moderate success in delaying or preventing the need for surgery.
Related: Yoga vs. Physical Therapy for Back Pain: What Science Actually Says
Surgery vs. Waiting: What Is Better?
If conservative treatment fails after six weeks, surgery becomes a consideration. But does surgery actually provide a better outcome than waiting it out?
A classic, long-term study reviewed in Clinical Orthopaedics and Related Research followed patients with lumbar disc herniations for an entire decade. The researchers found that patients who chose surgery experienced much faster pain relief and returned to work sooner than those who waited.
However, by the four-year mark, the patients who stuck with conservative treatment had caught up. At the ten-year mark, there was no significant difference in pain or mobility between the surgical group and the non-surgical group.
In short, surgery reliably speeds up recovery, but it does not necessarily change the long-term outcome.

Comparing Surgical Options
If surgery is chosen, the goal is always to remove the piece of the disc that is pressing on the nerve. Today, there are several ways to do this, ranging from traditional open surgery to minimally invasive techniques.
Many patients wonder if the newest, least invasive technique is the best. A massive 2025 analysis in Orthopadie looked at over 39,000 patients who had surgery for a lumbar herniated disc. They compared three popular methods:
1. Microdiscectomy: Using a microscope and a small incision.
2. Endoscopic microdiscectomy: Using a tiny camera through a tube.
3. Classical operation: A traditional open surgery.
The results were surprisingly consistent. Across all three methods, approximately 79% of patients reported good or excellent long-term results. The researchers concluded that no single operative procedure gave a superior long-term outcome. The choice of surgery should depend more on the specific location of the disc and the surgeon’s expertise.
Newer Minimally Invasive Alternatives
Scientists are also testing percutaneous treatments, which are procedures done through a needle without a surgical incision.
For example, a 2025 study in Pain Medicine evaluated percutaneous laser disc decompression (PLDD). The researchers found that using a laser to vaporize a small amount of the disc interior significantly reduced the size of the herniation on MRI scans, offering a viable option for patients who want to avoid open surgery.
However, not all needle-based treatments work well for everyone. A study in the Journal of Spinal Disorders & Techniques tested a procedure called nucleoplasty, which uses radio waves to dissolve disc tissue. The results in this specific trial were poor, with only 1 out of 16 patients achieving significant pain relief. The researchers noted that these procedures are highly dependent on patient selection and generally only work for small, contained herniations.
Who Benefits Or Needs Caution
While waiting is safe for most people, certain symptoms require immediate medical attention.
Emergency Situations:
A 2016 review in La Revue du Praticien stresses that surgery is required urgently if a patient develops Cauda equina syndrome (KAW-duh ee-KWY-nuh). This happens when a large disc herniation compresses the bundle of nerves at the base of the spine, causing loss of bowel or bladder control, numbness in the groin, or severe, progressive leg weakness.
Adolescents:
Though rare, teenagers can get herniated discs. A 2017 study in the Journal of Back and Musculoskeletal Rehabilitation looked at 70 adolescents with the condition. The researchers found that both conservative care and surgery were highly effective, but they recommended surgery if the teen experienced severe pain lasting more than six weeks that disrupted their routine life.
Thoracic Herniations:
Herniated discs in the middle of the back (thoracic spine) are incredibly rare, accounting for less than 4% of all disc surgeries. According to a 2018 review in Orthopaedics & Traumatology, these require special caution. Because the spinal cord is very vulnerable in this area, thoracic surgeries are technically difficult. Giant, calcified herniations in this area almost always require specialized surgical approaches to prevent spinal cord damage.
Common Questions About Herniated Discs
Does a larger herniation mean I will have a worse outcome?
Surprisingly, no. Research shows that massive, extruded disc herniations often shrink faster and more completely than smaller bulges. Because a large piece of disc material is so obviously out of place, the immune system mounts a stronger response to dissolve it.
Is a herniated disc the same as spinal stenosis?
No. A herniated disc is a localized injury where disc material spills out. Spinal stenosis is a gradual narrowing of the spinal canal, usually caused by bone spurs and thickened ligaments associated with aging.
Related: Treating Lumbar Spinal Stenosis: What the Latest Science Says
The Bottom Line
The science surrounding herniated disc treatment offers a very reassuring message: the body is highly capable of healing itself.
For the vast majority of patients without severe nerve damage, waiting four to six weeks while utilizing physical therapy and pain management is the most evidence-based approach. If symptoms refuse to budge, surgery is a highly effective way to speed up recovery.
Whether you opt for a traditional microdiscectomy or a newer endoscopic approach, the long-term success rates hover around 80%. Ultimately, the best treatment plan is one that aligns with your specific symptoms, the anatomy of your herniation, and your personal recovery goals.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| Long-Term Surgical Outcomes | Analysis of 39,000+ patients showed microdiscectomy, endoscopic, and classical surgeries all yield ~79% good/excellent long-term results. | PMID 39613966 |
| Laser Decompression | Percutaneous laser disc decompression (PLDD) significantly reduced herniated disc size on MRI. | PMID 40418221 |
| Surgery vs. Waiting | Surgery provides faster pain relief, but 4 to 10-year outcomes are nearly identical to conservative physical therapy. | PMID 16462442 |
| Exercise Therapy | Active cervical exercises (flexion, retraction) physically increased nerve space and improved symptoms in 8 weeks. | PMID 35906546 |
| Adolescent Herniations | Teens respond well to both conservative and surgical care; surgery is recommended for progressive weakness or pain >6 weeks. | PMID 27858699 |
Last updated: March 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.

Leave a Reply