
Imagine waking up with an ache in your lower back that shoots down your legs. You notice the pain gets worse when you stand or walk through the grocery store, but it magically fades when you sit down or lean forward over your shopping cart.
If this sounds familiar, you might be dealing with a condition called lumbar spinal stenosis. It affects hundreds of thousands of older adults every year.
When faced with this diagnosis, many people assume they need major spine surgery to fix the problem. However, the latest medical research paints a much more complicated picture. For most people, starting with conservative treatments like physical therapy and medication is the safest approach. Studies show that surgery carries higher risks without always providing better long-term relief compared to non-surgical care.
Here is a breakdown of what the latest scientific evidence actually says about treating lumbar spinal stenosis, from physical therapy to minimally invasive surgery.
Understanding Lumbar Spinal Stenosis
Your spine is made up of stacked bones called vertebrae. Down the middle of these bones runs a hollow space called the spinal canal, which protects your spinal cord and the bundle of nerves traveling to your legs.
As we age, the wear and tear on our bodies can cause the ligaments in our back to thicken, the discs between our bones to bulge, and arthritis to form bone spurs. All of this extra material takes up space.
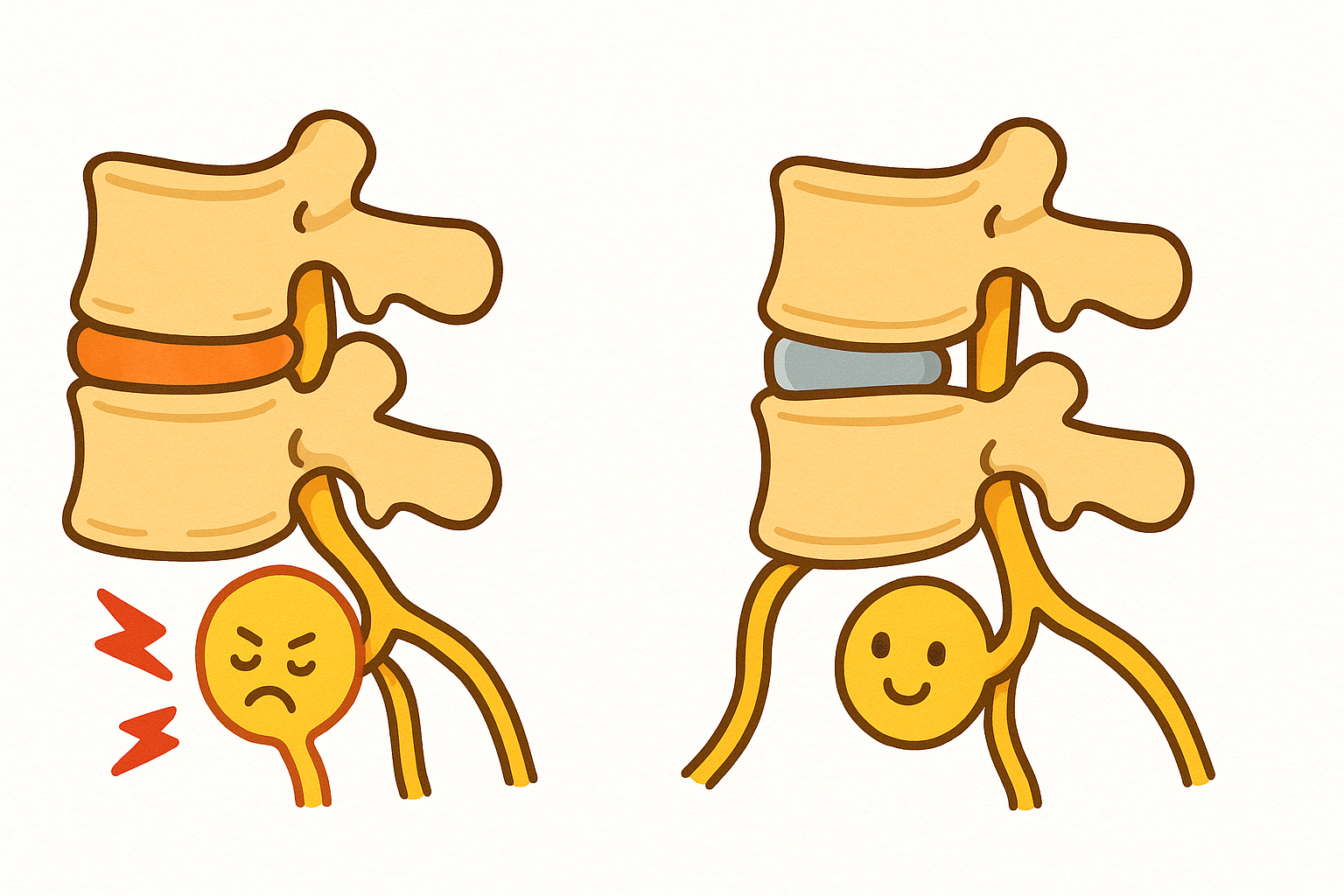
Lumbar spinal stenosis happens when that space narrows so much that it pinches the nerves in your lower back. You can think of it like a kink in a garden hose. When the hose is pinched, the water cannot flow properly. When your spinal nerves are pinched, the electrical signals to your legs are disrupted.
This pinching leads to a hallmark symptom called neurogenic claudication (noo-roh-JEN-ik klaw-dih-KAY-shun). This is a medical term for pain, cramping, or weakness in the legs that happens when you stand or walk.
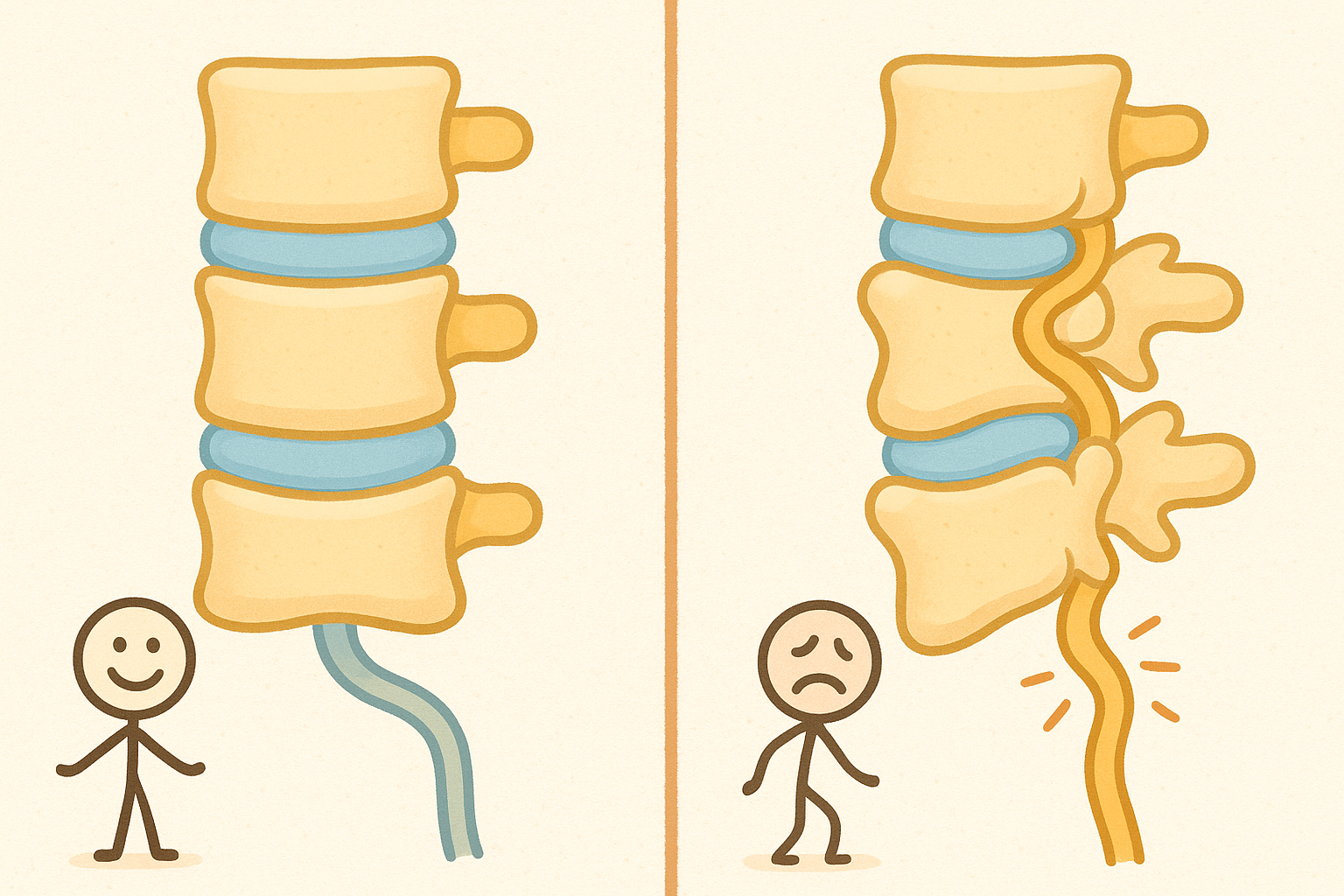
Interestingly, leaning forward or sitting down opens up the spinal canal just enough to un-kink the nerves, which is why people with this condition often lean on shopping carts or walkers for relief.

The MRI Disconnect
One of the most confusing aspects of lumbar spinal stenosis is that a picture of your spine does not always match how you feel.
A 2019 review in Der Orthopade noted that the findings on a magnetic resonance imaging (MRI) scan often do not correlate with a patient’s actual symptoms. Some people have MRI results showing severe narrowing but feel absolutely fine. Others have mild narrowing on an MRI but experience intense pain. Because of this, doctors treat the patient and their symptoms, not just the scan.
Does Surgery Actually Work Better Than Conservative Care?
When nerves are physically pinched by bone and tissue, it seems logical that cutting away the blockage would be the best solution. However, large reviews of the scientific literature show that the answer is not that simple.
A major 2016 review in The Cochrane database of systematic reviews looked at multiple trials comparing surgical treatments to non-surgical treatments. The researchers concluded that there is no clear benefit to choosing surgery over conservative care.
In fact, the review highlighted a significant difference in risks. The patients who received conservative treatment reported zero side effects. Meanwhile, the patients who underwent surgery experienced complication rates ranging from 10% to 24%. These complications included infections, bleeding, and nerve damage.
A 2021 review in The Spine Journal looked at how clinical guidelines are created for this condition. The researchers found that while many medical guidelines endorse surgery and injections, the actual scientific evidence supporting these interventions is quite poor.
Because the evidence does not firmly crown surgery as the winner, most medical guidelines recommend starting with conservative, non-surgical treatments.
First-Line Defenses: Non-Surgical Treatments
If you and your doctor decide to delay or avoid surgery, there are several ways to manage the pain and improve your ability to walk.
Physical Therapy and Exercise
Targeted exercise is a cornerstone of conservative treatment. A physical therapist can teach you specific stretches and exercises that strengthen your core and back muscles. This helps support the spine and can slightly change your posture to open up the spinal canal.
Related: Yoga vs. Physical Therapy for Back Pain: What Science Actually Says
Medications
Over-the-counter pain relievers can help with mild symptoms. For nerve-specific pain, doctors sometimes prescribe medications that change how the brain processes nerve signals. A 2017 review in Current opinion in anaesthesiology noted that medications like gabapentin and pregabalin are frequently included in initial treatment plans to help calm irritated nerves.
Related: Treating Neuropathic Pain: What the Latest Science Says
Epidural Steroid Injections
If physical therapy and oral medications are not enough, doctors may offer an epidural steroid injection. This involves using an X-ray to guide a needle into the spine and bathing the pinched nerves in a strong anti-inflammatory medication.
A 2012 review in the journal Spine found very low-quality evidence suggesting these injections can improve pain and function for up to two weeks compared to just resting. They do not fix the underlying narrowing, but they can provide a window of pain relief that allows a person to participate in physical therapy.
The Surgical Options: When Conservative Care Fails
If you have tried physical therapy, medications, and injections for several months without relief, or if your leg weakness is becoming severe, your doctor might suggest surgery.
The main goal of surgery is to decompress the nerves. This is typically done through a procedure called a laminectomy (lam-ih-NEK-tuh-mee). The surgeon removes the lamina, which is the bony roof covering the spinal canal, along with any thickened ligaments or bone spurs.
Open Surgery vs. Minimally Invasive Surgery
Historically, a laminectomy required a large incision down the back, known as open surgery. While effective at relieving pressure, open surgery can damage the muscles and structures that keep the spine stable.
To solve this problem, surgeons have developed minimally invasive techniques. A 2022 review in Medicina looked closely at a technique called microendoscopic decompression. Instead of a large cut, the surgeon uses a series of small tubes to gently separate the back muscles. They then use a tiny camera and specialized tools to remove the bone spurs.
Studies show that minimally invasive techniques offer similar pain relief to open surgery, but with less blood loss, shorter hospital stays, and less damage to the surrounding muscles. However, minimally invasive surgery is highly technical, and the surgeon must be very experienced to avoid complications like tearing the protective sac around the spinal nerves.
When Fusion is Necessary
Sometimes, the spine is not just narrow, it is also unstable. This often happens due to a condition called spondylolisthesis (spon-dih-low-lis-THEE-sis), which occurs when one vertebra slips forward over the bone below it.
A 2019 review in Neurosurgery Clinics of North America explains that if a patient has a slipped vertebra and spinal instability, a surgeon might need to perform a spinal fusion along with the decompression. This involves using screws and rods to lock the wobbly bones together.
Interspinous Spacers
Another option for some patients is an interspinous spacer. Because symptoms improve when a person leans forward, scientists designed small devices that can be wedged between the bones in the back of the spine.
A 2010 review in Pain Physician describes how devices like the X-STOP spacer force the spine into a slightly flexed position, opening up the spinal canal. A 2015 study in Expert review of medical devices compared a spacer to traditional decompression surgery. The researchers found that patients with the spacer had slightly better improvements in pain and physical function at 24 months, offering a less invasive alternative for the right candidates.
Alternative and Emerging Treatments
Researchers are always looking for new ways to treat back pain. One unique approach being studied is called acupotomy, also known as needle-knife therapy.
Acupotomy combines traditional acupuncture with a tiny scalpel attached to the tip of the needle. A 2019 meta-analysis in Medicine reviewed seven trials using this technique. The idea is that the tiny blade can release tight muscles and ligaments around the spine. The researchers found that acupotomy improved pain and function better than standard acupuncture or physical traction. However, the study authors cautioned that the quality of the research was low, and more rigorous testing is needed before it becomes a mainstream recommendation.
Common Questions About Lumbar Spinal Stenosis
Does a bad MRI mean I will eventually need surgery?
No. Research shows that MRI images do not perfectly predict how much pain you will have. Many people live with narrow spinal canals and manage their symptoms well with physical therapy and occasional medications.
Will my condition just keep getting worse?
Spinal stenosis is a degenerative condition, meaning it is linked to aging. However, the symptoms often wax and wane. You might have a bad flare-up for a few weeks, followed by months of manageable symptoms. It does not always progress to the point of severe disability.
Is it bad to walk if it causes pain?
Walking is generally good for your overall health. If walking causes severe leg pain, you should stop and rest. Physical therapists often recommend walking in shorter bursts, using a rolling walker, or trying a stationary bike, which naturally puts your spine in a comfortable, leaning-forward position.
The Bottom Line
Lumbar spinal stenosis is a common cause of leg and back pain in older adults, but a diagnosis does not automatically mean you need an operation.
- What we know: For most people, conservative treatments like physical therapy, targeted exercises, and medications should be the first step.
- What remains uncertain: High-quality research has not proven that surgery is universally better than conservative care in the long run.
- How to proceed: If non-surgical treatments fail after several months, or if your symptoms are severely limiting your life, surgery is a valid option. Minimally invasive techniques and spacers offer promising alternatives to traditional open surgery, though they require highly skilled surgeons.
Discuss your specific symptoms, your daily limitations, and your tolerance for surgical risks with your healthcare provider to build a plan that works for you.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| Surgical vs. Non-Surgical Care | Low-quality evidence shows no clear benefit of surgery over conservative care, but surgery carries higher complication risks. | PMID 26824399 |
| Minimally Invasive Surgery | Microendoscopic decompression provides similar outcomes to open surgery with less blood loss and shorter hospital stays. | PMID 35334560 |
| Clinical Guidelines | Most medical guidelines recommend surgery and injections, despite the underlying evidence being of poor quality. | PMID 33122056 |
| Interspinous Spacers | Spacers that keep the spine slightly flexed showed durable symptom relief compared to standard decompression at 24 months. | PMID 26487285 |
| Acupotomy (Needle-Knife) | Early research suggests acupotomy may improve pain and function, but high-quality safety data is still needed. | PMID 31393365 |
Last updated: March 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.



Leave a Reply