
Hearing a doctor say you have “cysts” on your ovaries can sound alarming. For many people, the word cyst brings to mind a harmful growth that might require surgery. However, the cysts associated with Polycystic Ovary Syndrome (PCOS) are entirely different.
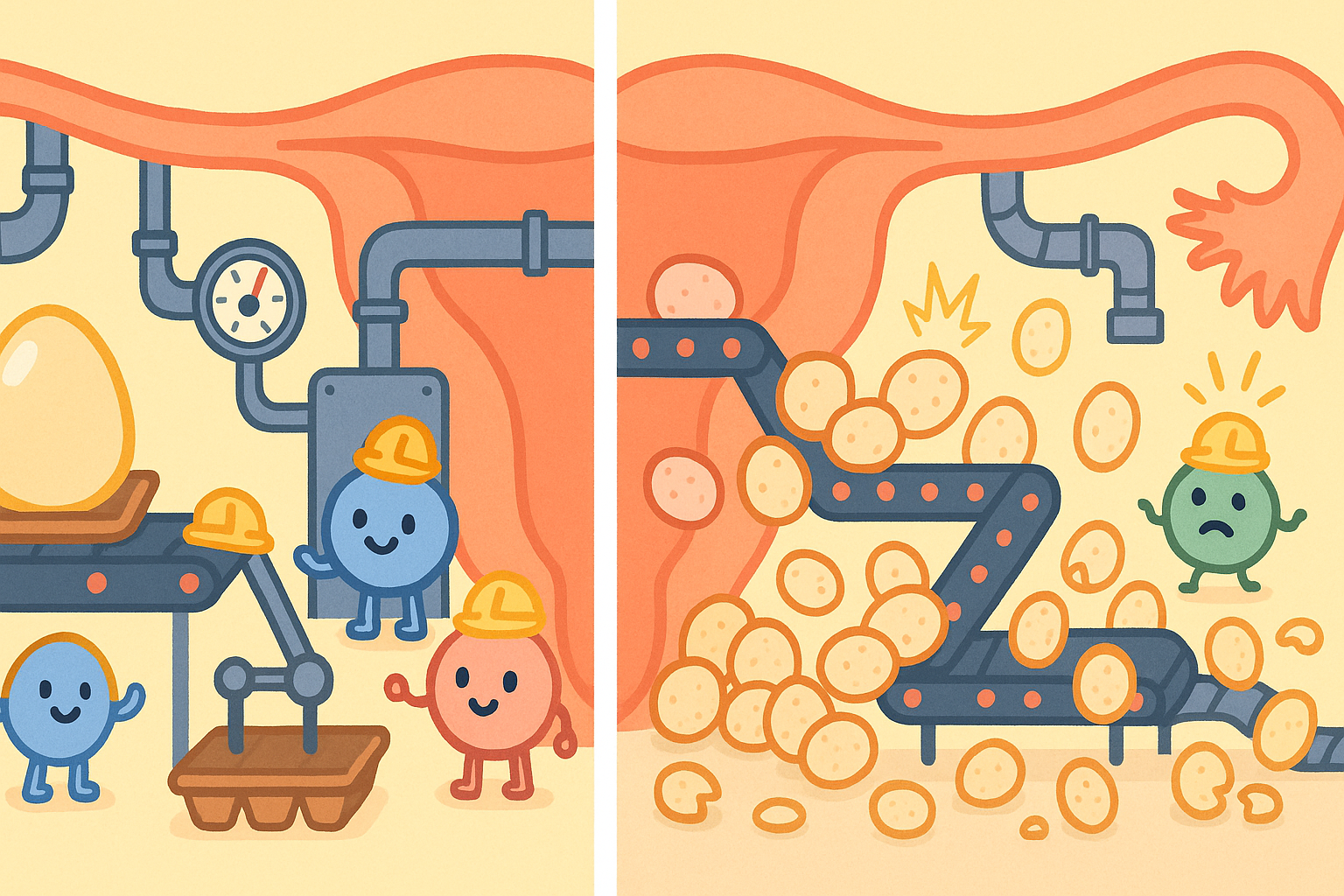
Think of the ovary as a factory that is supposed to produce one finished product (a mature egg) each month. In a person with PCOS, the factory receives confusing chemical signals. Instead of focusing on one product, the factory starts working on dozens of eggs at once. Because the signals are unbalanced, the factory never finishes any of them. These unfinished egg sacs simply pile up along the edges of the ovary.
This article explains exactly what these cysts are, why they form, and what the latest peer-reviewed research says about managing the root causes of PCOS.
What Are the “Cysts” in Polycystic Ovary Syndrome?
To understand PCOS, we first need to understand what the “cysts” actually are. In a healthy menstrual cycle, an egg grows inside a tiny fluid-filled sac called a follicle. Once the egg is mature, the follicle bursts open to release it. This is called ovulation.
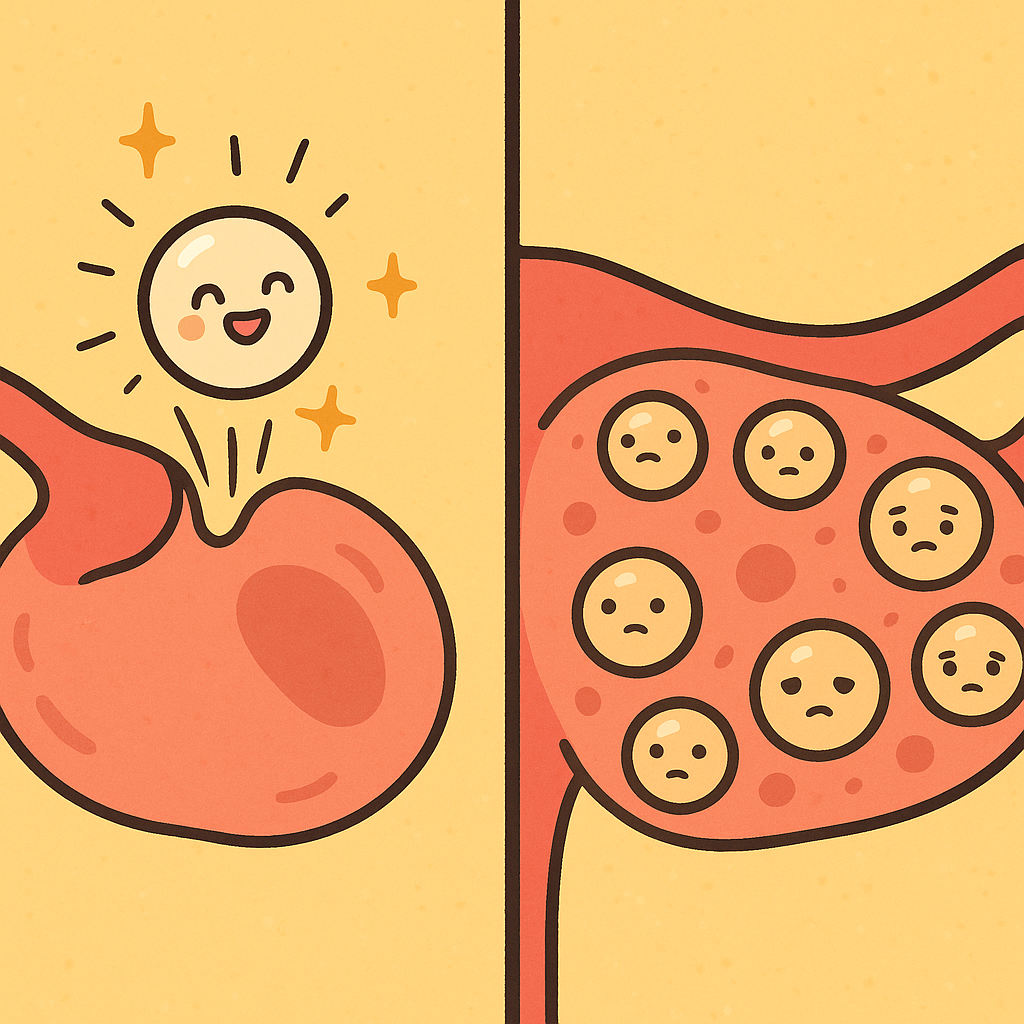
In PCOS, the hormonal signals required to trigger ovulation are disrupted. Because the eggs never fully mature, the follicles never burst. They remain on the ovary as small, paused fluid-filled sacs. Therefore, the “cysts” in PCOS are simply normal, immature egg follicles that stopped growing halfway through the process.
A 2025 review in the Journal of Ovarian Research notes that these accumulated follicles are a hallmark of the condition, leading to the “polycystic” appearance on an ultrasound. They are not tumors, and they do not typically require surgical removal.
Common Questions About PCOS Cysts
Are PCOS cysts dangerous?
No. The follicles themselves are harmless. They are a symptom of an underlying hormonal imbalance, not a disease on their own.
Do these cysts cause pelvic pain?
Unlike classic ovarian cysts (which can grow very large and cause severe pain or rupture), the small immature follicles in PCOS generally do not cause acute pelvic pain. If a person with PCOS experiences sudden, severe pelvic pain, it is usually due to a different issue.
Do they go away?
Yes. When the underlying hormonal and metabolic imbalances are treated, normal ovulation can resume, and the accumulation of these paused follicles often resolves.
How This Might Work: Why Do These “Cysts” Form?
To understand why the ovary factory gets confused, we have to look at the body’s chemical messengers. PCOS is driven by a complex web of hormones that miscommunicate.
The Brain-Ovary Connection
The brain controls the ovaries using two main hormones: Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). FSH tells the ovary to grow a follicle, and a spike in LH tells the ovary to release the egg.
Research shows that people with PCOS often have an elevated ratio of LH to FSH. According to a 2024 review in The Journal of Endocrinology, the brain sends too much LH and not enough FSH. Without enough FSH, the follicle cannot mature. The constant high levels of LH instead tell the ovaries to produce extra male hormones.
Hyperandrogenism and Insulin Resistance
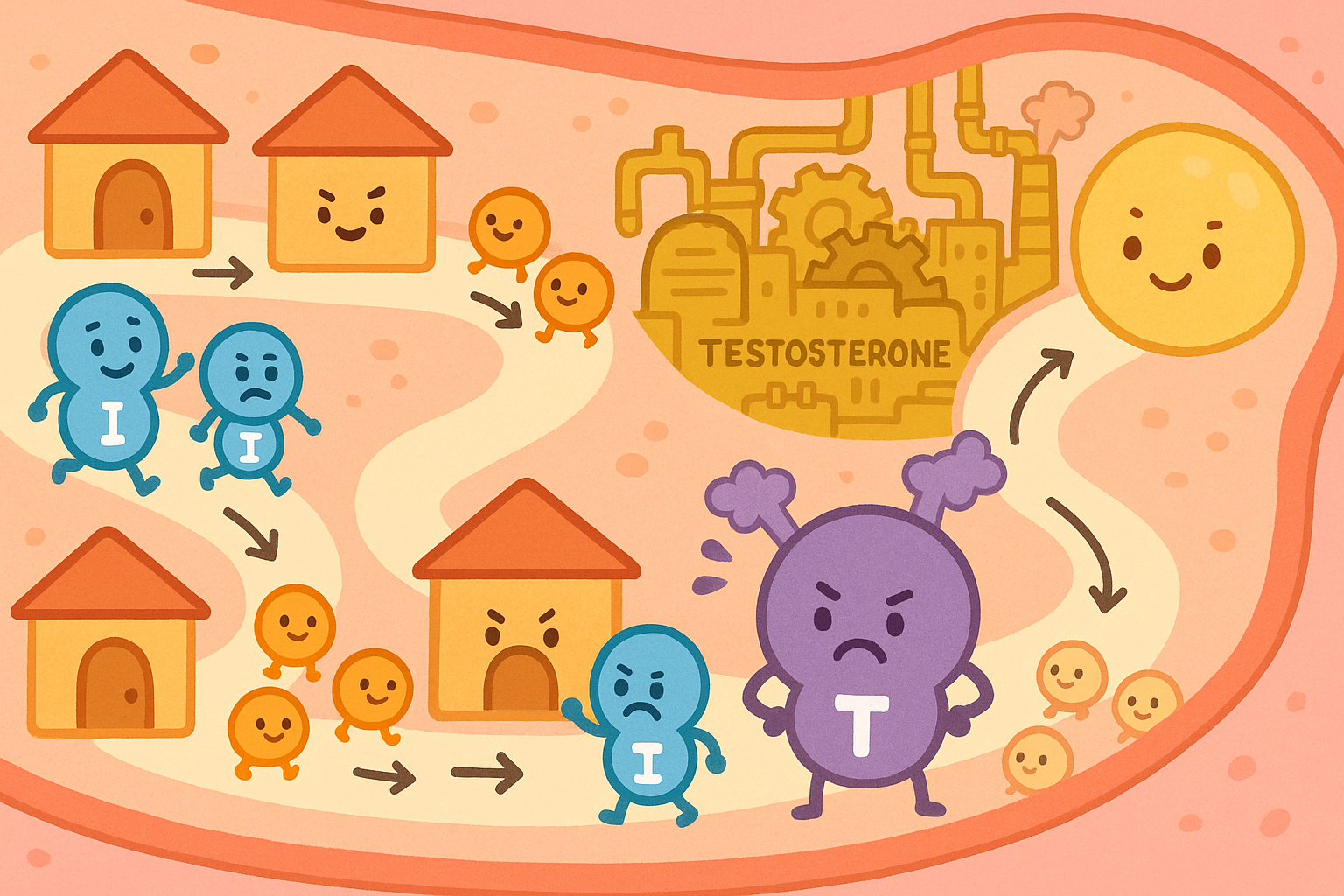
Hyperandrogenism (HI-per-an-DROJ-en-izm) is a condition where the body produces higher-than-normal levels of male hormones, like testosterone. This is a primary driver of PCOS. It causes physical symptoms like excess facial hair, acne, and hair thinning.
But what causes the ovaries to produce extra testosterone? In many cases, the culprit is insulin resistance (IN-suh-lin ree-ZIS-tuhns). This happens when the body’s cells stop responding properly to insulin, a hormone that regulates blood sugar. To compensate, the body pumps out even more insulin.
A 2021 review in the Archives of Gynecology and Obstetrics explains that high insulin levels directly stimulate the ovaries to produce more testosterone. This excess testosterone acts like a roadblock in the ovary, preventing the follicles from maturing and leading to the buildup of “cysts.”
Cellular Energy Problems
Recent science is also looking at the microscopic power plants inside our cells, called mitochondria. A 2020 study in the International Journal of Molecular Sciences found that the cells surrounding the eggs in PCOS patients often have mitochondrial dysfunction. When these cells cannot produce enough energy, they cannot process hormones correctly, which further stalls egg development.
What the Research Shows: A Full-Body Condition
While the name “Polycystic Ovary Syndrome” focuses on the ovaries, modern science recognizes it as a systemic, full-body metabolic and inflammatory condition.
The Gut Microbiome Connection
One of the most heavily researched areas in recent years is the connection between PCOS and the gut microbiome (the trillions of bacteria living in your digestive tract).
Scientists have proposed the “DOGMA” theory (Dysbiosis of Gut Microbiota). A 2020 review in the Journal of the American College of Nutrition explains that an imbalance in gut bacteria can cause the intestinal lining to become slightly “leaky.” This allows bacterial toxins to enter the bloodstream, triggering the immune system. This chronic, low-grade inflammation worsens insulin resistance, which in turn drives up testosterone production and stops ovulation.
A 2022 mouse study in Gut Microbes found that PCOS alters specific gut bacteria, such as decreasing Bacteroides acidifaciens. Interestingly, researchers found that diet had a massive impact on these bacteria. Intermittent Fasting: What the Latest Science Actually Says is one area of dietary research being explored to manage this insulin and gut relationship.
The Immune System and Thyroid Overlap
PCOS is closely linked to how the immune system functions. A 2024 genetic study in the International Journal of Surgery found clear genetic links between specific immune cell behaviors and the development of ovarian cysts and PCOS.
Because the immune system is hyperactive, people with PCOS are also at a higher risk for autoimmune conditions. A 2023 review in Frontiers in Endocrinology highlighted that women with PCOS have a significantly higher risk of developing autoimmune thyroiditis (Hashimoto’s disease) and subclinical hypothyroidism. When the thyroid slows down, it can further disrupt the menstrual cycle and worsen metabolic symptoms.
Long-Term Metabolic Risks
Because PCOS is rooted in metabolism, it carries long-term risks if left unmanaged. According to a 2022 study in Life Sciences, women with PCOS have a notably higher risk of developing gestational diabetes during pregnancy. What Science Actually Says About Managing Gestational Diabetes is an important topic for anyone with PCOS planning to conceive. Furthermore, the condition increases the lifetime risk of type 2 diabetes and cardiovascular disease.
Who Benefits Or Needs Caution
While PCOS shares common traits, it does not look the same in everyone. Research clearly identifies distinct populations that experience the condition differently.
Lean PCOS vs. Obese PCOS
While obesity worsens insulin resistance, not everyone with PCOS is overweight. About 20-30% of people with the condition have “Lean PCOS.”
A 2021 study in the Journal of the College of Physicians and Surgeons Pakistan compared hormone levels between these groups. Researchers found that a specific adrenal hormone called DHEAS was significantly higher in people with Lean PCOS compared to those with Obese PCOS. This suggests that Lean PCOS might be driven more by adrenal gland stress than by severe insulin resistance, meaning treatment approaches may need to differ based on body type.
Mental Health Considerations
The physical symptoms of PCOS can take a heavy toll on mental well-being. A 2022 study in Reproductive Sciences assessed psychological distress in women with PCOS. The researchers found that patients dealing with severe hirsutism (excess body hair) were three times more likely to experience high levels of anxiety. Patients dealing with higher body weights were more likely to experience obsessive thoughts. Healthcare providers are increasingly urged to treat the psychological impacts of PCOS alongside the physical symptoms.
Practical Guidance: How Science Approaches Treatment
Because PCOS is a full-body condition, treating the “cysts” means treating the underlying metabolic and hormonal environment.
Diet and Lifestyle Modifications
The most effective first-line approach to managing PCOS is lifestyle adjustment. A 2022 review in the Journal of Food Biochemistry outlined that a balanced diet focusing on low-glycemic carbohydrates, high protein, and healthy fats (like omega-3s from walnuts and fish) can drastically improve symptoms.
For those who are overweight, losing just 5-10% of body weight can be enough to lower insulin levels, reduce testosterone, and restart normal ovulation. For patients struggling with severe insulin resistance, doctors sometimes prescribe medications that help the body process glucose. GLP-1 Weight Loss Drugs: What Real-World Results Actually Show is a growing area of interest for managing the metabolic side of PCOS.
Medical Options for Ovulation
For patients trying to conceive, doctors often use medications to force the ovaries to mature an egg, overriding the hormonal roadblocks.
Historically, a drug called Clomiphene citrate was the standard treatment. However, newer science points to an alternative. A 2023 randomized controlled trial in the Journal of Medicine and Life compared Clomiphene to a drug called Letrozole.
| Measurement | Letrozole Group | Clomiphene Group |
|---|---|---|
| Ovulation Rate | 86.0% | 72.0% |
| Pregnancy Rate | 22.0% | 18.0% |
| Time to Ovulation | 17.2 days | 24.0 days |
The study found that Letrozole resulted in a significantly shorter time to ovulation and a slightly higher overall ovulation rate, making it a highly effective option for fertility treatment in PCOS.
Emerging Therapies: Probiotics
Because of the gut microbiome connection, scientists are testing probiotics as a treatment for PCOS. A 2025 study in BMC Complementary Medicine and Therapies tested a probiotic mixture on a rat model of PCOS. The researchers found that the probiotics reduced ovarian cysts, lowered testosterone, and decreased inflammation. While human trials are still ongoing, supporting gut health through fermented foods and fiber is a low-risk strategy with high potential benefits.
The Bottom Line / Takeaways
- The cysts are not tumors: The “cysts” in PCOS are actually paused, immature egg follicles that failed to ovulate due to hormonal imbalances.
- It is a full-body condition: PCOS is driven by a combination of insulin resistance, high male hormones, chronic inflammation, and altered gut bacteria.
- Metabolic health is key: Managing insulin through diet, exercise, and sometimes medication is the most effective way to reduce testosterone and restore normal ovulation.
- Fertility is possible: While PCOS is a leading cause of infertility, medications like Letrozole have proven highly effective at helping patients ovulate and conceive.
- The evidence is strong: The scientific community is highly confident that addressing the metabolic and inflammatory roots of PCOS is the safest and most sustainable way to manage the condition long-term.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| PCOS Physiology | High LH/FSH ratios and insulin resistance drive the accumulation of immature follicles in the ovaries. | PMID 39980043 |
| Gut Microbiome | Gut dysbiosis triggers systemic inflammation, worsening insulin resistance and hyperandrogenism in PCOS. | PMID 31513473 |
| Fertility Treatments | Letrozole resulted in a faster time to ovulation compared to Clomiphene in women with PCOS. | PMID 37520487 |
| Thyroid Overlap | Women with PCOS face a significantly higher risk of developing autoimmune thyroiditis and hypothyroidism. | PMID 37635968 |
| Mental Health | Physical symptoms of PCOS, specifically hirsutism, are strongly correlated with elevated clinical anxiety. | PMID 34642910 |
| Lean vs. Obese PCOS | Lean PCOS patients showed significantly higher levels of the adrenal hormone DHEAS compared to obese patients. | PMID 33775010 |
Last updated: March 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.

Leave a Reply