Why Standard Cholesterol Tests Do Not Tell the Whole Story
If you want to know your risk for a heart attack, your doctor will likely order a standard lipid panel to check your cholesterol. This is a highly effective way to measure your metabolic health. However, a standard cholesterol test has a blind spot. It only tells you if you have the “ingredients” for heart disease floating in your blood. It does not tell you if those ingredients have actually started sticking to your artery walls.
Imagine hiring a home inspector who only looks at the building materials in your driveway, rather than checking the actual pipes inside the walls.
This is where a Coronary Artery Calcium scan comes in. Often referred to as a CAC score, this test is a specialized, low-dose CT scan of your heart. Instead of guessing your risk based on blood markers, it takes a direct picture of your coronary arteries to look for physical evidence of disease.
By understanding what this test measures, who should get it, and what the numbers mean, you can make more informed decisions about your long-term heart health.
How This Might Work: The Biology of Heart Plaque
To understand what a calcium score is actually measuring, we have to look at how heart disease develops over time.
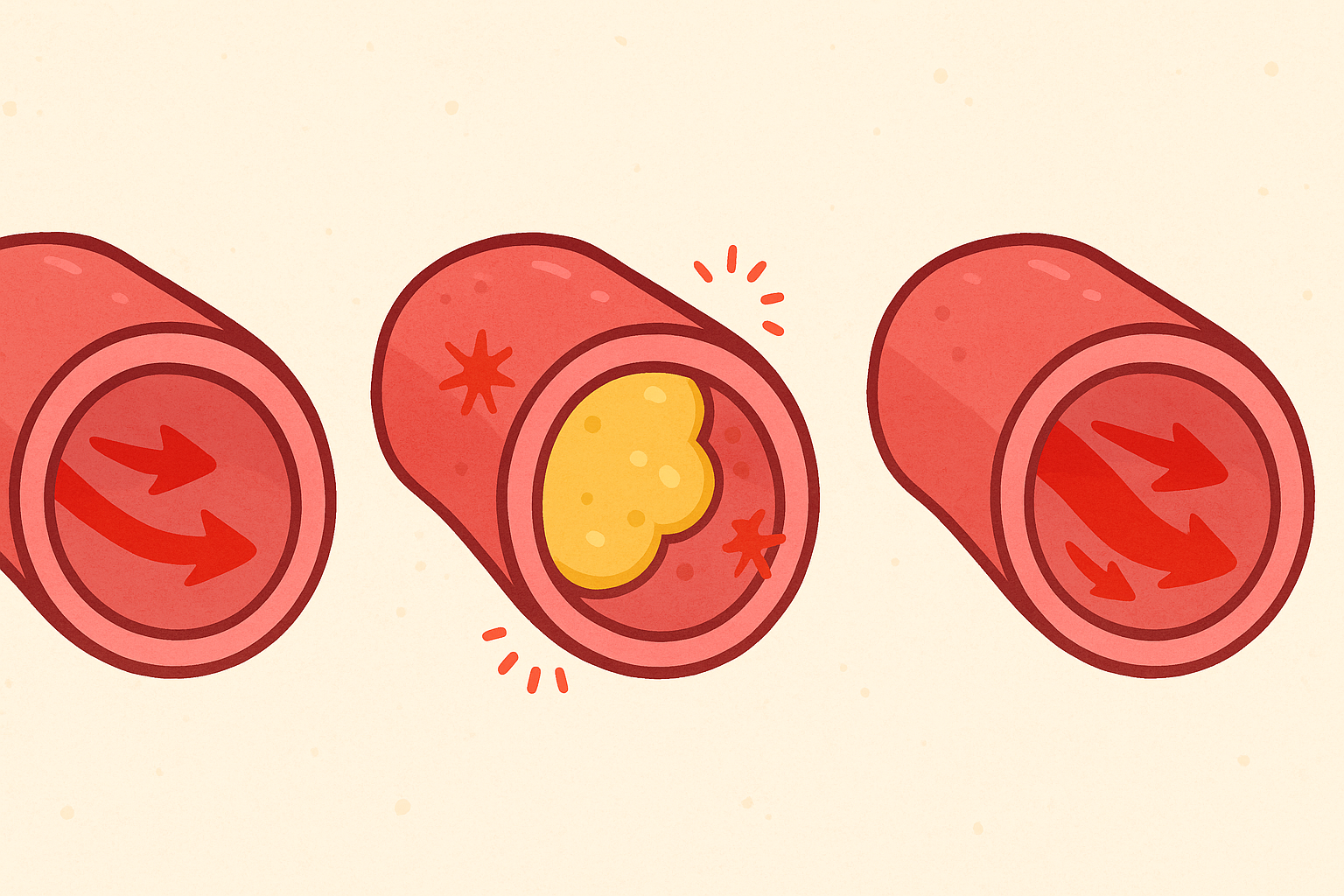
Heart attacks are usually caused by Atherosclerosis (ath-er-o-skluh-RO-sis), which is a condition where fatty deposits called plaque build up inside your artery walls. In the early stages, this plaque is soft, unstable, and highly inflammatory. Soft plaque is dangerous because it can easily rupture. If it ruptures, a blood clot forms to seal the wound, and that clot can block blood flow to the heart.
Your body knows that soft plaque is dangerous. To protect you, your immune system tries to heal the area by covering the soft plaque with a hard, bone-like shell. This healing process is called Calcification (kal-sih-fih-KAY-shun).
Think of calcification like a scab forming over a deep cut. The calcium itself is not what causes a heart attack. In fact, calcified plaque is more stable and less likely to rupture than soft plaque. However, the presence of calcium is a permanent footprint. It proves that dangerous soft plaque was there in the first place.
The CAC scan uses X-rays to spot these dense, calcified “scabs” in your heart’s arteries. The more calcium the scanner sees, the more plaque your body has had to heal over the years.
What the Research Shows: The MESA Study
For decades, scientists debated the best way to predict heart attacks. The turning point for the CAC score came from a massive, long-term research project called the Multi-Ethnic Study of Atherosclerosis, widely known as the MESA study.
Starting in the year 2000, researchers tracked over 6,800 men and women across the United States. They gave everyone a CAC scan and then monitored their health for over a decade. The results completely changed how cardiologists view preventive heart care.
A 2008 study in The New England Journal of Medicine detailing the MESA findings showed that a person’s calcium score was a much stronger predictor of future heart events than traditional risk factors like high cholesterol or high blood pressure alone.
Researchers found two major patterns:
1. The Power of Zero: People with a score of zero had an incredibly low risk of suffering a heart attack over the next 10 years, even if they had high cholesterol.
2. The Danger of High Scores: People with high calcium scores (above 300) had a significantly higher risk of heart attacks, even if their cholesterol levels looked normal on paper.
A more recent 2021 review in the Journal of the American College of Cardiology confirmed these findings, noting that the CAC score is currently the most accurate tool doctors have to decide if a patient actually needs to take cholesterol-lowering medication.
Decoding Your Results: What the Numbers Mean
When you get a CAC scan, the results are calculated using the Agatston scoring system. This system measures both the density and the total area of the calcium deposits in your arteries.
Your final report will usually provide two numbers. The first is your absolute score. The second is your percentile, which compares your score to other people of your exact age, gender, and ethnicity.
Here is a general breakdown of what the absolute scores mean:
| CAC Score | Level of Disease | Estimated 10-Year Heart Risk | Medical Consensus for Action |
|---|---|---|---|
| 0 | No visible hard plaque | Very Low | Maintain healthy lifestyle. Re-test in 3 to 5 years. |
| 1 to 99 | Mild disease | Low to Moderate | Focus on diet and exercise. Statins may be considered based on other risks. |
| 100 to 399 | Moderate disease | High | Statins are strongly recommended. Daily aspirin may be discussed. |
| 400 or higher | Severe disease | Very High | Aggressive cholesterol lowering, strict lifestyle changes, and possible stress testing. |
It is important to remember that the percentile matters just as much as the absolute score. A score of 50 is fairly normal for an 80-year-old man. However, a score of 50 in a 45-year-old woman is highly unusual and places her in a high-risk percentile, requiring immediate medical attention.
Common Misunderstandings About Calcium Scores
Because this test deals with the heart, it is easy to misinterpret the results. There are several common myths that research has clearly debunked.
Myth 1: You can lower your calcium score with diet and supplements.
Once calcium is deposited in your artery walls, it is effectively permanent. You cannot dissolve it with vitamins, special diets, or medications. However, the goal is not to lower the score. The goal is to stop the score from going up rapidly. If you are interested in how plaque behaves over time, you can read more about Can You Actually Reverse Arterial Plaque? What the Latest Science Says.
Myth 2: Statins will lower your calcium score.
This is perhaps the most surprising scientific finding for many patients. If you start taking a statin (a cholesterol-lowering drug), your calcium score might actually go up faster than it would have without the drug.
This sounds alarming, but it is actually a good thing. Statins pull the dangerous, inflammatory fat out of your soft plaque. As the fat leaves, the body fills the empty space with dense calcium to stabilize the area. A rising calcium score while on a statin often means the drug is working to harden and secure your plaque so it does not rupture.
Myth 3: A score of zero means you are completely immune to heart attacks.
A score of zero is excellent news, but it is not a perfect guarantee. The scanner only sees hard, calcified plaque. It cannot see new, soft plaque. If you have a very recent buildup of soft plaque, your score will be zero, but you still carry some risk. This is why doctors still look at your overall lifestyle and blood pressure.
Who Benefits Or Needs Caution
Medical guidelines are very clear about who should get this test and who should skip it.
Who Benefits Most:
- People with “Intermediate” Risk: If you are between 40 and 75 years old and your doctor is unsure if you need a statin, this test is the ultimate tiebreaker.
- People with a Family History: If you have a parent or sibling who had an early heart attack, a CAC score can reveal if you are inheriting that same risk.
- People Hesitant About Medication: If you prefer not to take daily medication, a score of zero can safely allow you to delay starting a statin for several years.
Who Should Skip It:
- People Who Already Had a Heart Attack or Stent: We already know you have severe heart disease. The scan will not provide any new information, and the metal from a stent will blind the scanner anyway.
- Young People at Low Risk: If you are under 40 with normal cholesterol and no family history, your score will almost certainly be zero. The test is an unnecessary expense and exposes you to unneeded radiation.
- People Already on High-Dose Statins: If you are already doing everything medically possible to protect your heart, knowing your exact score will not change your treatment plan.
How This Compares To Alternatives
When assessing heart risk, doctors have a few different tools. Here is how the CAC score compares to other common tests:
- Standard Lipid Panel (Cholesterol Test): Cheap, widely available, and requires a blood draw. It is great for general screening but cannot confirm if plaque actually exists.
- Coronary Artery Calcium (CAC) Scan: Costs around $100 to $200 (often not covered by insurance). Takes 10 minutes, requires no needles, and directly measures hard plaque. It exposes you to a very small amount of radiation, roughly equal to a mammogram.
- Coronary CTA (Computed Tomography Angiography): A much more advanced and expensive CT scan that uses an injected contrast dye. Unlike the basic CAC scan, a CTA can see both hard calcium AND dangerous soft plaque. It is usually reserved for people actively experiencing chest pain.
Practical Guidance: What to Do If Your Score Is High
If you receive a high calcium score, it is normal to feel anxious. However, a high score is not a death sentence. It is an early warning system that gives you time to act.
Research strongly supports the following steps if your score is elevated:
1. Discuss Statin Therapy: The clinical consensus is that patients with a score over 100 benefit significantly from statins, which lower cholesterol and stabilize existing plaque.
2. Control Blood Pressure: High blood pressure acts like a hammer, pounding against your artery walls and making plaque more likely to rupture. Keeping blood pressure in a normal range is critical.
3. Monitor Blood Sugar: High blood sugar damages the lining of your arteries, accelerating plaque growth. Improving metabolic health is key. For more on tracking this, see Continuous Glucose Monitors: What the Latest Science Actually Says.
4. Consider a Daily Aspirin: For scores over 100, some doctors recommend a low-dose aspirin to prevent blood clots, though this depends entirely on your personal bleeding risk.
Common Questions About Coronary Calcium Scores
Do I need to fast before the test?
No. Because the test is an X-ray picture of your heart and not a blood test, you can eat and drink normally beforehand.
Does the test hurt or trigger claustrophobia?
No. There are no needles or IVs. You simply lie flat on a table while a donut-shaped scanner moves over your chest. Your head is completely outside the machine, so claustrophobia is rarely an issue.
Why doesn’t my insurance cover this test?
Despite strong backing from the American Heart Association, many insurance companies still classify the CAC score as a “screening” test rather than a “diagnostic” test, meaning they will not pay for it. Fortunately, most hospitals offer it out-of-pocket for a flat fee, usually between $99 and $150.
The Bottom Line
A Coronary Artery Calcium score is one of the most thoroughly researched and reliable tools for predicting heart disease. By taking a direct look at the calcified plaque in your arteries, it removes the guesswork from traditional cholesterol tests.
We know with high confidence that a score of zero indicates a very low risk of a heart attack in the near future. We also know that scores above 100 require proactive medical treatment to stabilize the arteries.
However, the test is not for everyone. It cannot see new soft plaque, and the score cannot be reversed once it goes up. If you are between the ages of 40 and 75 and are unsure about your true heart risk, a CAC scan can provide the clarity you and your doctor need to make the right choices for your longevity.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| MESA Study (10-Year Follow Up) | CAC score is a significantly stronger predictor of heart events than standard risk factors alone. | PMID 18378618 |
| Clinical Guidelines Review | CAC scoring is the preferred method to determine if intermediate-risk patients require statin therapy. | PMID 34412241 |
Last updated: March 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.
Leave a Reply