It is a classic story in sports medicine. A person is playing basketball, tennis, or softball. They step back to push off their foot and suddenly hear a loud “pop.” Many people describe feeling like someone kicked them in the back of the leg. They turn around to look, but no one is there.
This is the hallmark sign of an Achilles tendon rupture (uh-KILL-eez TEN-dun RUP-chur).
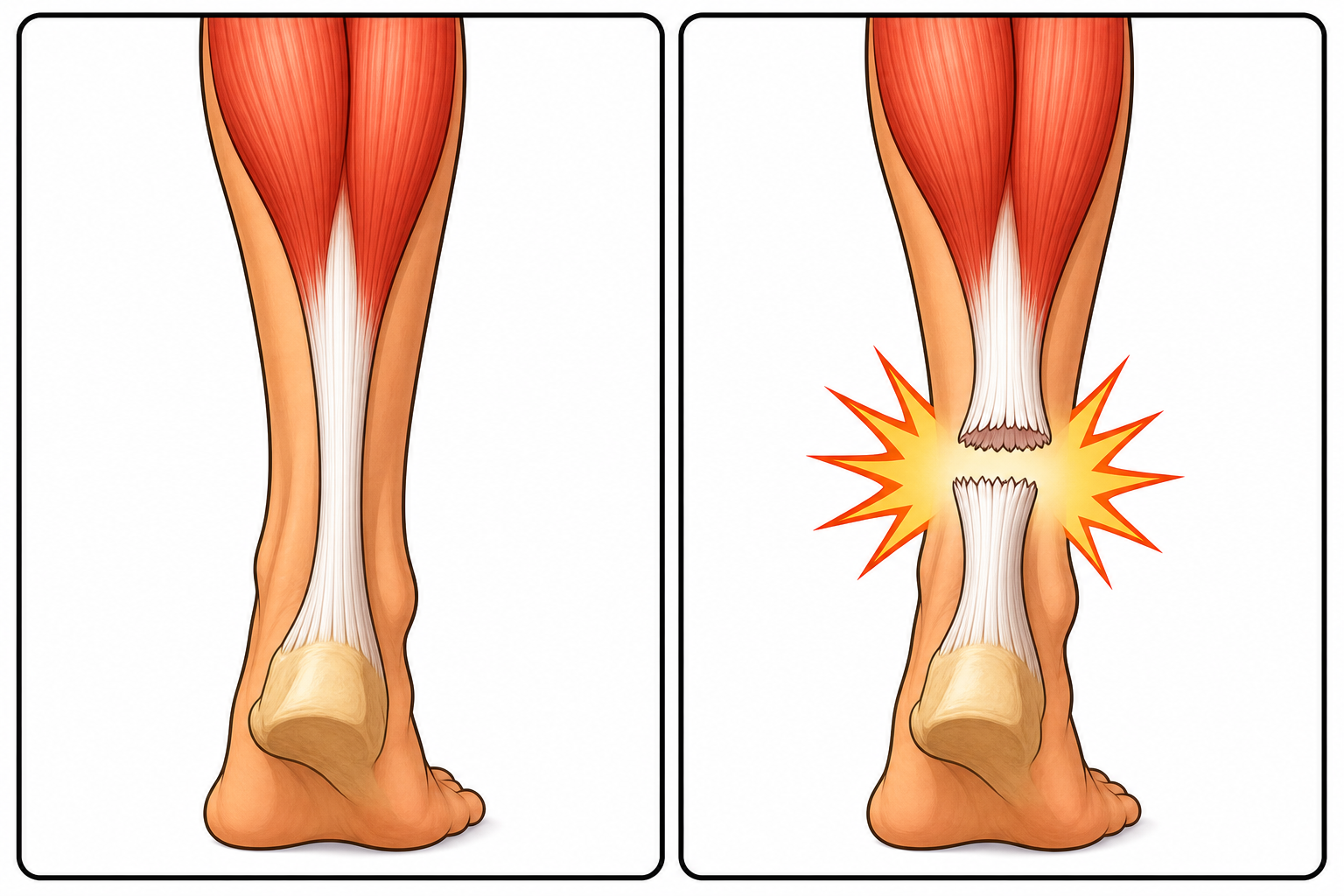
The Achilles is the thick cord of tissue that connects your calf muscles to your heel bone. It is the strongest and thickest tendon in the human body. Every time you walk, jump, or run, this tendon absorbs massive amounts of force. When that force becomes too much, the tendon can snap.
For decades, the standard medical response to a ruptured Achilles was immediate surgery. However, recent scientific studies have sparked a major debate in orthopedics. Researchers are now finding that for many people, skipping surgery and using a specific type of physical therapy might work just as well.
In this article, we will explore what peer-reviewed research actually says about how the Achilles ruptures, who is most at risk, and whether surgery is truly necessary for a full recovery. Related: The Science of Achilles Tendon Injuries and Recovery
Who Is Most at Risk for a Rupture?
While anyone can tear their Achilles, research shows clear patterns regarding who is most likely to suffer this injury.
The most common patient is often referred to as the “weekend warrior.” These are typically people in their 30s or 40s who have sedentary jobs during the week but engage in intense, stop-and-go sports on the weekends.
According to a 2013 study in Foot & Ankle International, this injury is heavily skewed toward men. Researchers reviewed 358 acute ruptures and found that men accounted for 302 of them, creating a male-to-female ratio of more than 5 to 1. The average age for these acute ruptures was about 43 years old.
However, there are exceptions in specific athletic populations. A 2022 study in Sports Health looked at female collegiate gymnasts. The researchers found that the risk of Achilles rupture in women’s gymnastics is 10 times higher than in all other collegiate sports combined. Gymnasts who competed at elite levels, performed highly difficult tumbling passes, and trained heavily were at the highest risk.
What Actually Happens Inside the Leg?
When a doctor evaluates a torn Achilles, they look at the “morphology” of the tear, which means the physical shape and location of the damage.
A 2021 study in The Journal of Foot and Ankle Surgery evaluated 220 acute ruptures during surgery to see exactly how the tendon breaks. The findings were remarkably consistent:
- Complete tears are the norm: 98.7% of the injuries were complete ruptures, meaning the tendon snapped entirely in two. Only 1.3% were partial tears.
- Location matters: 95% of the ruptures happened in the “mid-substance” of the tendon. This is the middle area of the cord, roughly a few inches above the heel bone. This area naturally has a poorer blood supply, making it more vulnerable to injury and slower to heal.
- The break is usually clean: 90% of the tears had a transverse pattern, meaning the tendon snapped straight across horizontally.
Common Misunderstandings About Tendon Ruptures
A very common myth is that an Achilles tendon will always warn you before it breaks. Many people assume that a rupture is the final result of months of chronic pain or stiffness.
It is true that tendinopathy (ten-dih-NOP-uh-thee) is a major issue. This is a condition where the tendon suffers chronic wear, tear, and microscopic damage over time. However, a rupture does not always require prior damage.
A 2019 study in Knee Surgery, Sports Traumatology, Arthroscopy examined the tissue of 152 ruptured Achilles tendons under a microscope. While 77% of the tendons showed signs of prior chronic damage, a surprising 23% of the ruptured tendons were completely healthy before they snapped.
The researchers noted that healthy tendons were more likely to rupture in patients who had lower overall sports activity levels or who suffered a non-sports-related accident (like missing a step on a staircase). In short, you do not need to have a history of heel pain to suffer a sudden rupture.
The Great Debate: Surgery vs. Non-Surgical Treatment
If you rupture your Achilles today, your doctor will present you with two main paths: operative (surgery) or non-operative (conservative treatment).
Historically, doctors believed that surgery was the only way to prevent the tendon from healing too loosely or tearing again. Today, the science is much more nuanced.
The Non-Surgical Approach (Functional Rehabilitation)
Conservative treatment used to mean putting the leg in a hard cast for months. This caused the calf muscle to waste away and left the ankle extremely stiff.
Modern non-surgical treatment relies on functional rehabilitation. Instead of a rigid cast, the patient wears a specialized walking boot with wedges under the heel. These wedges point the toes downward, bringing the two torn ends of the tendon close together so they can heal naturally. Over several weeks, the wedges are slowly removed to stretch the tendon back to its normal length.

A 2019 review in Foot and Ankle Clinics found that when early functional rehabilitation is used, non-surgical patients achieve outcomes very similar to surgical patients.
The Surgical Approach
Surgery involves making an incision in the back of the leg and physically stitching the two ends of the tendon back together.
According to a 2015 systematic review in the Scandinavian Journal of Medicine & Science in Sports, both treatments have pros and cons. The review looked at 10 years of randomized controlled trials and found:
- There was no statistically significant difference in re-rupture rates between the two groups, though there was a slight trend favoring surgery.
- Surgery patients generally returned to work slightly faster.
- Surgery carries unique risks, specifically skin infections and wound healing problems at the incision site.
The researchers concluded that the quality of the physical therapy and rehabilitation program might actually be more important than whether a surgeon stitches the tendon or not. Related: The Science of Athletic Injury Recovery: What Actually Works
Comparing the Two Paths
| Feature | Surgical Treatment | Non-Surgical (Functional Rehab) |
|---|---|---|
| Best Suited For | Young, elite athletes; delayed diagnoses | Older adults; sedentary individuals; those with health risks |
| Infection Risk | Higher (due to surgical incision) | Very low (no incision) |
| Re-rupture Risk | Slightly lower | Slightly higher (especially if patient is non-compliant) |
| Tendon Strength | Highly reliable tension | Risk of the tendon healing slightly elongated |
If Surgery Is Chosen: Open vs. Percutaneous
If a patient and doctor decide on surgery, there is another choice to make regarding the surgical technique.
1. Open Repair: The surgeon makes a long vertical cut down the back of the calf to fully expose the tendon. This allows for a very strong repair but increases the risk of the skin failing to heal properly.
2. Percutaneous Repair (per-kyoo-TAY-nee-us): The surgeon makes several tiny pokes in the skin and threads the sutures through the tendon using specialized tools.
A 2013 review in Foot and Ankle Clinics highlights that percutaneous repair significantly reduces the risk of superficial skin breakdown and wound problems compared to open surgery, while still providing a strong repair.
The Healing Timeline: Why Patience Is Mandatory
Whether treated with surgery or a boot, recovering from an Achilles rupture is a notoriously long and frustrating process.
Patients often wonder why they cannot return to sports after a few months. A fascinating 2018 study in The American Journal of Sports Medicine tracked exactly what happens to the tendon during the first year of recovery.
Researchers placed tiny metal beads inside the tendons of 75 surgical patients. By taking specialized X-rays over time, they could measure exactly how much the tendon stretched as it healed. They divided the patients into groups, allowing some to put weight on their foot immediately, while others were completely restricted from walking for 7 weeks.
The results were surprising:
- The rehabilitation rules during the first 8 weeks (early walking vs. no walking) did not significantly alter how much the tendon stretched.
- The Achilles tendon continued to elongate and stretch for up to 6 full months after surgery.
- Muscle strength, endurance, and patient-reported function did not return to normal values even at the 12-month mark.
This research underscores a vital biological reality: tendons heal much slower than muscles or bones. Because they have limited blood flow, building new, strong collagen fibers takes a minimum of one year.
Acute vs. Chronic Ruptures: When Waiting Is Dangerous
The debate between surgery and non-surgical treatment only applies to acute ruptures (injuries diagnosed and treated within the first few days).
Sometimes, a person ruptures their Achilles but does not realize it. Because other lower leg muscles can still point the foot downward slightly, some people assume they just suffered a severe calf cramp or sprain. If the injury is not diagnosed for more than 4 to 6 weeks, it is classified as a chronic or neglected rupture.
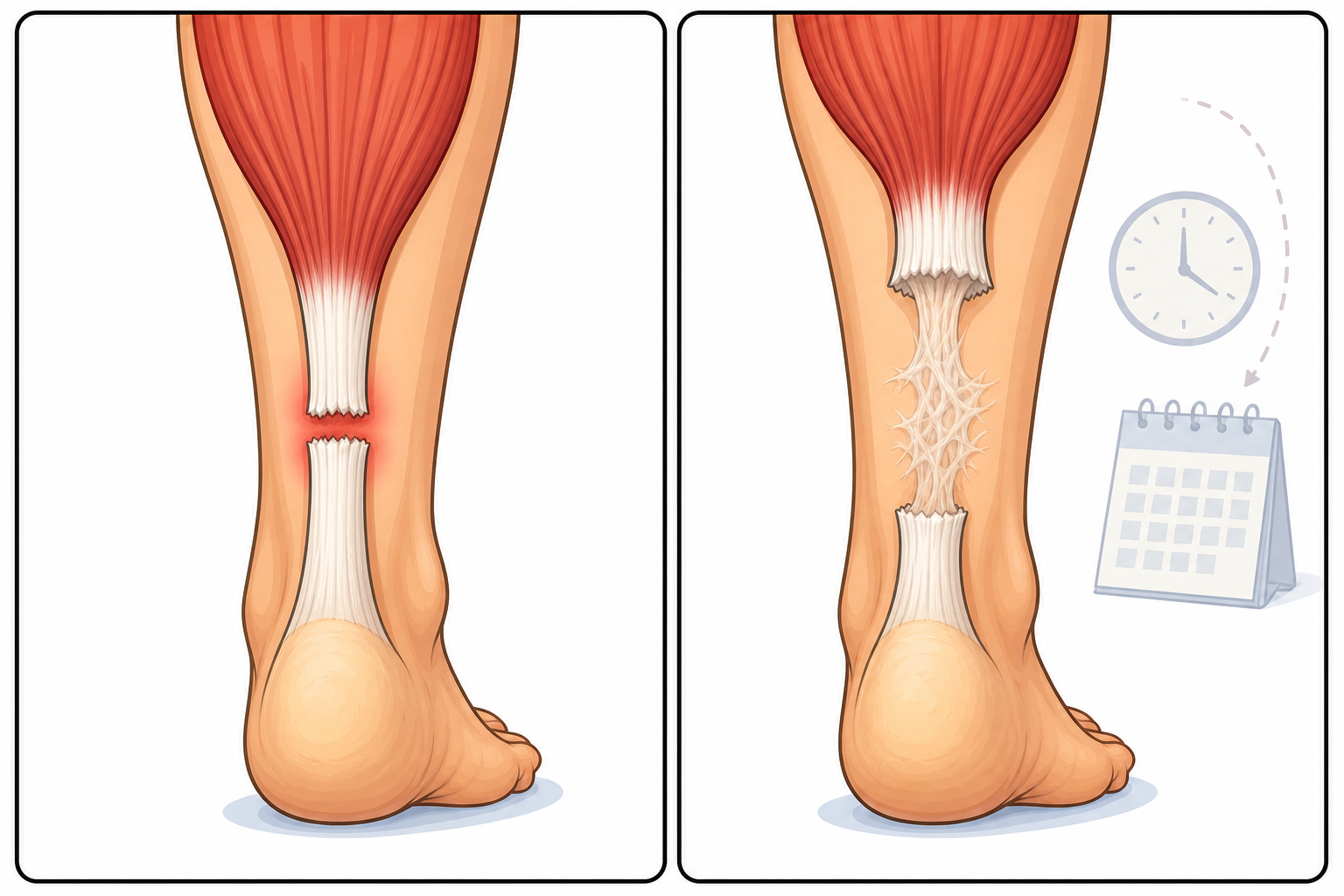
According to a 2025 review in Clinics in Podiatric Medicine and Surgery, chronic ruptures are a much more complex medical problem. Over a few weeks, the calf muscle pulls the upper half of the snapped tendon high up into the leg. The gap between the two torn ends becomes too large to heal on its own, and the space fills with weak scar tissue.
A 2012 study notes that non-surgical treatment is rarely an option for neglected ruptures. Surgeons usually have to perform complex reconstruction, which may involve lengthening the calf muscle (gastrocnemius advancement) or transferring a tendon from the big toe to help support the heel.
The Bottom Line
The science of Achilles tendon ruptures has evolved significantly over the last decade. Here is what the current evidence tells us:
- It can happen to anyone: While middle-aged men playing weekend sports are the most common demographic, elite athletes and even sedentary people can suffer a rupture.
- Warning signs are not required: Nearly a quarter of all ruptures happen to tendons that were perfectly healthy the day before.
- Surgery is no longer mandatory for everyone: High-quality, functional rehabilitation in a walking boot provides outcomes very similar to surgery for the average person.
- Athletes often still choose surgery: Operative repair remains the preferred choice for young, highly active individuals who need guaranteed tendon tension for explosive jumping and sprinting.
- Recovery is a one-year commitment: Tendons take up to 6 months to stop stretching and at least 12 months to regain normal strength, regardless of the treatment chosen.
If you suspect you have torn your Achilles, the most critical step is seeking immediate medical attention. The sooner the foot is stabilized, the better the chances the tendon will heal properly, whether a surgeon stitches it or your body repairs it naturally.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| Tendon Elongation | The Achilles elongates for 6 months post-surgery; full recovery takes at least 12 months. | PMID 29965789 |
| Treatment Comparison | Functional rehabilitation yields similar outcomes to surgery, but surgery has a slightly lower re-rupture rate. | PMID 24650079 |
| Prior Damage | 23% of ruptured Achilles tendons showed no signs of prior chronic damage or tendinosis. | PMID 30267184 |
| Demographics | Acute ruptures are roughly 5.4 times more common in men than women, averaging 43 years of age. | PMID 23386761 |
| Tear Morphology | 98.7% of surgical cases were complete ruptures, mostly in the mid-substance of the tendon. | PMID 34134918 |
| Chronic Ruptures | Delays in diagnosis beyond 4-6 weeks require complex surgical reconstruction. | PMID 40483025 |
Last updated: June 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen or making decisions about injury treatment.


Leave a Reply