
For many parents, introducing solid foods to an infant comes with a quiet sense of anxiety. What if they react to peanut butter? What if cow’s milk causes a rash? These fears are common, and for good reason. Food allergies in children have become a significant public health focus over the last few decades, with prevalence rising in industrialized nations.
At its core, a food allergy is an error made by the immune system. The body mistakenly identifies a harmless food protein as a dangerous invader and launches a defense to attack it. This reaction can range from mild hives to severe, life-threatening breathing difficulties.
However, the scientific understanding of food allergies has shifted dramatically in recent years. We now know that not all food allergies work the same way, that blood tests are not always accurate predictors of severe reactions, and that the old advice to delay feeding infants potential allergens was likely incorrect.
This article synthesizes the latest peer-reviewed research to explain how childhood food allergies work, how they are diagnosed, and what science actually says about preventing and managing them.
Common Questions About Food Allergies
Is a food intolerance the same as a food allergy?
No. A food intolerance (like lactose intolerance) happens in the digestive system when the body cannot break down a food properly. A food allergy involves the immune system and can cause reactions throughout the entire body.
Does delaying allergenic foods prevent allergies?
Research shows the opposite is true. Introducing highly allergenic foods like peanuts and eggs early (around 4 to 6 months of age) actually helps train the immune system to tolerate them.
Do children outgrow their food allergies?
It depends on the food. Allergies to cow’s milk, egg, wheat, and soy are frequently outgrown during childhood. Allergies to peanuts, tree nuts, fish, and shellfish are much more likely to persist into adulthood.
How This Might Work: The Immune System Mistake
To understand food allergies, it helps to look at the cells responsible for the reaction. The immune system is like a complex security network designed to keep pathogens like viruses and bacteria out. In a child with a food allergy, this security system flags a benign food protein as a threat.
There are two main categories of food allergies, and they operate using different biological mechanisms.
IgE-Mediated Food Allergies
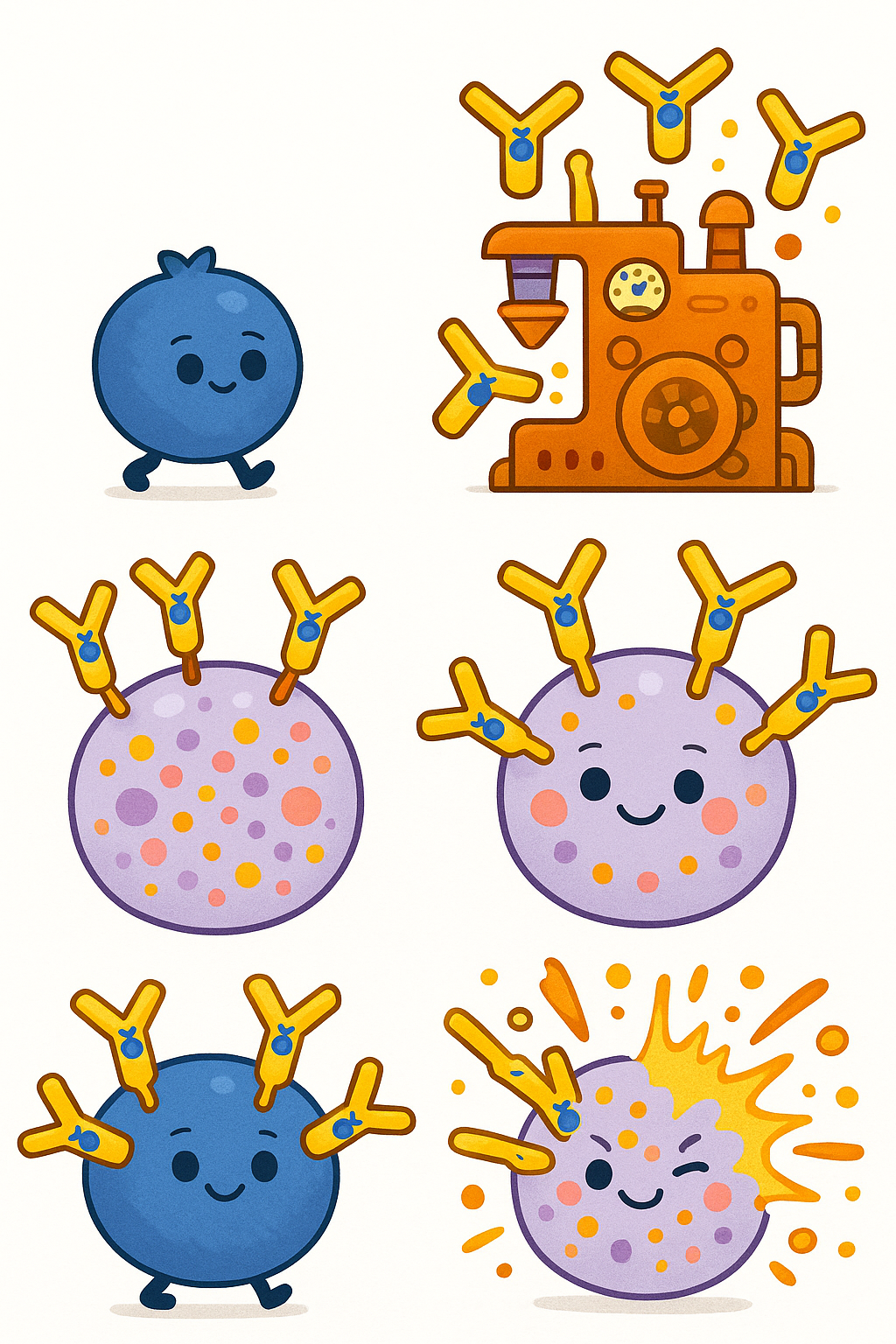
This is the classic, rapid-onset food allergy. It involves an antibody called Immunoglobulin E (im-yoo-noh-GLOB-yoo-lin ee), or IgE for short.
When a child is first exposed to a food, their immune system might mistakenly create IgE antibodies specific to that food protein. This process is called Sensitization (sen-sih-tih-ZAY-shun). These IgE antibodies attach themselves to Mast cells (MAST sells), which are immune cells located in the skin, respiratory tract, and gut.
If the child eats that food again, the proteins bind to the IgE antibodies on the mast cells. This causes the mast cells to break open and release a flood of chemicals, including histamine. According to a 2019 review in Clinical Reviews in Allergy & Immunology, this chemical release happens within minutes to a few hours, causing immediate symptoms like hives, swelling, vomiting, or breathing trouble.
Non-IgE-Mediated Food Allergies
Not all food allergies involve IgE antibodies. Non-IgE-mediated allergies involve different parts of the immune system, primarily T-cells.
Because they do not rely on the rapid release of histamine, these reactions are delayed. Symptoms might not appear until hours or even days after the food is eaten. A 2020 review in Nutrients explains that these allergies mostly affect the gastrointestinal tract, causing chronic vomiting, diarrhea, or poor growth.
One of the most well-known non-IgE conditions is FPIES (Food Protein-Induced Enterocolitis Syndrome). Enterocolitis (en-ter-oh-coh-LYE-tis) refers to inflammation of the small and large intestines. FPIES typically presents in infancy with profuse, repetitive vomiting a few hours after consuming triggers like cow’s milk, soy, or rice.
| Feature | IgE-Mediated Allergy | Non-IgE-Mediated Allergy |
|---|---|---|
| Immune Mechanism | IgE antibodies and mast cells | T-cells and other immune cells |
| Timing of Symptoms | Minutes to 2 hours | Hours to days |
| Common Symptoms | Hives, swelling, wheezing, anaphylaxis | Vomiting, bloody stools, chronic diarrhea |
| Common Triggers | Peanut, tree nuts, milk, egg, shellfish | Cow’s milk, soy, rice, oats |
What the Research Shows About Common Allergens
While any food can theoretically trigger an allergic reaction, a small group of foods is responsible for the vast majority of cases. A 2020 review in Pediatric Annals notes that eight foods account for most serious allergic reactions: cow’s milk, eggs, fish, crustacean shellfish, wheat, soy, peanuts, and tree nuts.
The Natural History of Food Allergies
One of the most frequent questions parents ask is whether their child will have this allergy forever. The answer depends heavily on the specific food involved.
A 2024 review in Current Allergy and Asthma Reports outlines the typical “natural history” (how a disease progresses over time) of childhood food allergies.
Research consistently shows that allergies to cow’s milk, egg, soy, and wheat usually develop in infancy and often resolve by the time the child reaches school age. For example, about 50 percent of children outgrow an egg allergy by age three to five.
Conversely, allergies to peanuts, tree nuts, fish, and shellfish tend to develop slightly later in early childhood and are much more stubborn. Only about 20 percent of children with a peanut allergy will eventually outgrow it.
Common Misunderstandings About Diagnosis
Diagnosing a food allergy is more complex than simply running a blood test. A common misunderstanding among parents (and sometimes healthcare providers) is that a positive allergy test means a child cannot eat a specific food.
According to a 2020 review in Medicina, skin prick tests and blood tests look for the presence of specific IgE antibodies. However, having these antibodies only proves that the body is sensitized to the food. It does not guarantee that the child will actually have an allergic reaction when they eat it.
Many children have positive blood tests for foods they eat safely every day. Because these tests have a high rate of false positives, allergists warn against running large panels of food allergy tests without a clear history of a reaction. Doing so often leads to unnecessary dietary restrictions.
The gold standard for diagnosing a food allergy is the Oral Food Challenge (OFC). During an OFC, a child is given gradually increasing amounts of the suspected food in a strictly monitored medical setting. If the child eats a full serving without a reaction, the allergy is ruled out.
The Shift in Prevention: Why Early Introduction Matters
For many years, pediatric guidelines recommended that parents delay introducing highly allergenic foods to infants. Parents were told to wait until age one for cow’s milk, age two for eggs, and age three for peanuts and fish.
However, as these avoidance guidelines were widely adopted, the rates of food allergies actually increased.
Scientists began to investigate why this was happening. A landmark study published in 2015, known as the LEAP (Learning Early About Peanut Allergy) study, fundamentally changed how we view prevention. As detailed in a 2020 review in Pediatrics in Review, researchers found that introducing peanuts to high-risk infants between 4 and 11 months of age significantly reduced their risk of developing a peanut allergy by age five.

This led to the “dual-allergen exposure hypothesis.” This theory suggests that if a child’s first exposure to a food protein happens through the skin (especially inflamed skin, like eczema), the immune system sees it as an invader and develops an allergy. But if the first exposure happens through the digestive system, the gut trains the immune system to tolerate the food.
Today, guidelines strongly recommend the early introduction of potentially allergenic foods, particularly peanuts and eggs, starting around 4 to 6 months of age, to help prevent allergies from developing.
Hidden Impacts: Nutrition, Growth, and Mental Health
Managing a food allergy involves much more than avoiding a specific ingredient. The daily burden of navigating a restricted diet can have profound effects on a child’s physical and emotional well-being.
Nutritional Risks and Feeding Difficulties
When major food groups like dairy, wheat, or eggs are removed from a child’s diet, they are at risk for nutritional deficiencies. A 2024 study in The Journal of Allergy and Clinical Immunology: In Practice highlights that children with food allergies are at an increased risk for poor growth.
Furthermore, the anxiety surrounding food can alter a child’s relationship with eating. A 2024 report by the European Academy of Allergy and Clinical Immunology found that feeding difficulties, such as food refusal or lack of age-appropriate eating habits, are highly prevalent in children with food allergies, affecting up to 40 percent of those with multiple allergies.
Social and Economic Burdens
The social impact of food allergies is also significant. A 2023 study in Japan surveyed children with food allergies and found that 21 percent reported being bullied specifically because of their allergy. In some cases, children were coerced into touching or eating their allergens.
Financially, safe food alternatives are often more expensive. A 2022 paper in the Annals of Allergy, Asthma & Immunology emphasizes that food insecurity heavily impacts families managing food allergies. Specialized diets and hypoallergenic formulas place a heavy financial burden on low-income households, making it difficult to safely feed their children.
Where The Science Is Still Uncertain: Future Treatments
Currently, there is no cure for food allergies. The standard treatment is strict avoidance of the trigger food and carrying emergency medication, such as an epinephrine auto-injector, to treat accidental exposures.
However, science is actively exploring ways to rewire the immune system.
Oral Immunotherapy (OIT)
One of the most researched treatments is Oral Immunotherapy. This involves giving a child tiny, precisely measured, and gradually increasing doses of their allergen every day.
The goal is Desensitization (dee-sen-sih-tuh-ZAY-shun), which means raising the threshold of how much food the child can accidentally eat before having a reaction. According to a 2014 review in Current Pharmaceutical Design, OIT is effective at inducing desensitization, protecting children from severe reactions to accidental cross-contamination.
However, the science is still uncertain about whether OIT creates true, long-lasting tolerance. If a child stops eating their daily maintenance dose, the allergy often returns. OIT also carries a risk of allergic reactions during the treatment itself.
The Microbiome and Transplant-Acquired Allergies
Researchers are also learning how deeply the gut microbiome and the liver are involved in food tolerance. A fascinating, albeit rare, phenomenon known as Transplant-Acquired Food Allergy (TAFA) highlights this connection.
A 2024 review in Nutrients explains that some children who undergo solid organ transplants (particularly liver transplants) suddenly develop new food allergies. Scientists suspect this is due to a combination of immune-suppressing medications, the transfer of immune cells from the donor, and massive disruptions to the gut microbiome. Studying these rare cases is helping researchers better understand how the gut bacteria and the liver communicate with the immune system to build tolerance, which could eventually lead to new therapies for all food allergy sufferers.
Related: Probiotics and Gut Health: What the Science Actually Shows
The Bottom Line
Childhood food allergies represent a complex immune system error that requires careful management and vigilance.
What we know with high confidence:
- Food allergies are divided into rapid IgE-mediated reactions and delayed non-IgE-mediated reactions.
- Blood and skin tests are prone to false positives; an oral food challenge is the most accurate diagnostic tool.
- Early introduction of highly allergenic foods helps prevent allergies, completely reversing decades of previous medical advice.
- Allergies to milk and egg are frequently outgrown, while peanut and tree nut allergies usually persist.
What remains uncertain:
- While treatments like Oral Immunotherapy can temporarily desensitize the immune system, we do not yet know how to permanently cure an established food allergy.
- The exact reasons why food allergies have increased so rapidly over the last few decades are still being investigated, though changes in our environment, gut microbiome, and past delayed-feeding guidelines likely all play a role.
Managing a food allergy takes a village, from vigilant parents and educated teachers to supportive peers. As science continues to uncover exactly how the immune system learns to tolerate food, the future holds promise for better prevention and, eventually, lasting treatments.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| Natural History of Allergies | Milk, egg, and wheat allergies frequently resolve in childhood, while peanut and tree nut allergies often persist into adulthood. | PMID 38416390 |
| Allergy Prevention | Early introduction of highly allergenic foods is recommended to build immune tolerance, replacing old guidelines that suggested delaying introduction. | PMID 32737253 |
| Diagnostics | Skin prick and blood tests only show sensitization and have high false-positive rates; the Oral Food Challenge remains the gold standard for diagnosis. | PMID 32143431 |
| Non-IgE Allergies | Non-IgE allergies like FPIES cause delayed gastrointestinal symptoms and are frequently outgrown by age 3 to 5. | PMID 32674427 |
| Nutritional Impact | Children with food allergies are at high risk for growth deficiencies and require careful nutritional monitoring and dietary planning. | PMID 38280452 |
| Immunotherapy | Oral Immunotherapy (OIT) can successfully desensitize children to allergens, though long-term, permanent tolerance remains uncertain. | PMID 23701567 |
Last updated: May 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.



Leave a Reply