For decades, a standard cholesterol test has been the primary tool doctors use to assess heart health. You are likely familiar with the main numbers: total cholesterol, HDL (good) cholesterol, and LDL (bad) cholesterol. But what if the standard LDL number does not tell the whole story?
If you have been reading about heart health recently, you may have heard of a test called ApoB. Apolipoprotein B (uh-PAWL-ih-poh-PRO-teen B) is a protein that sits on the surface of every cholesterol particle that can cause plaque buildup in your arteries.
So, what is the difference between LDL and ApoB? A standard LDL test measures the total weight of the cholesterol carried in your blood. An ApoB test measures the actual number of particles carrying that cholesterol.
Research shows that knowing your particle count is often a more accurate predictor of heart disease and stroke risk than standard LDL cholesterol tests. This article explores what the latest science says about ApoB, how it compares to traditional tests, and who might benefit from knowing their number.
The Difference Between Cholesterol Weight and Particle Count
To understand why scientists are focusing on ApoB, it helps to use an analogy.
Imagine your bloodstream is a highway. The cholesterol molecules are passengers, and the lipoproteins (like LDL) are the cars carrying them.
A standard LDL cholesterol test weighs all the passengers in the cars. If the total weight is low, we assume the highway is safe. However, a low total weight could mean you have a few buses carrying a lot of passengers, or it could mean you have a massive fleet of tiny cars, each carrying only one or two passengers.
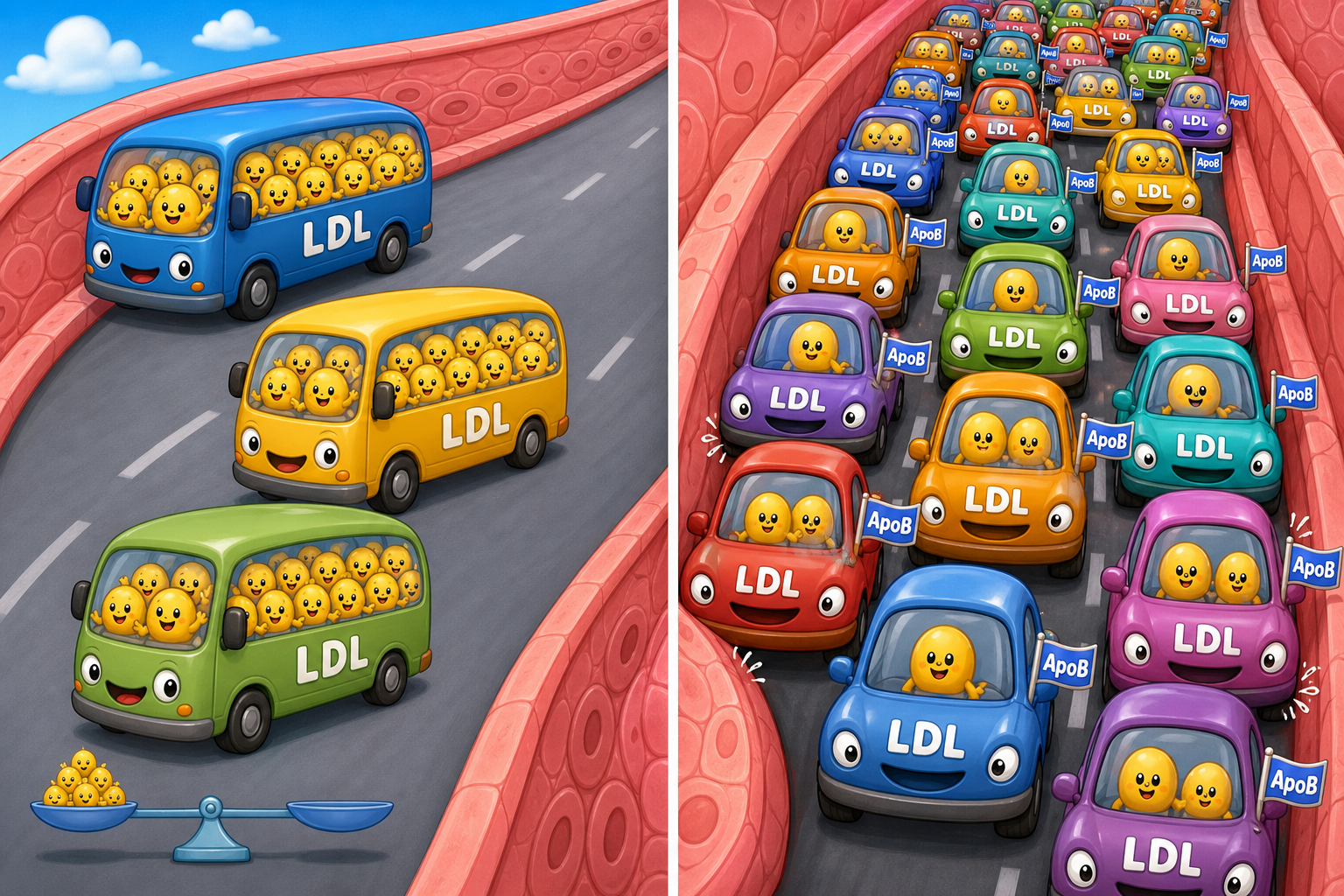
Artery damage does not happen because of the weight of the passengers. It happens when the cars crash into the walls of the highway (your blood vessels) and get stuck. The more cars on the road, the higher the chance of a crash.
Because there is exactly one ApoB protein on every single “car” that can cause plaque, measuring ApoB tells us exactly how much traffic is on your highway.
What the Research Shows About ApoB vs. LDL-C
A large body of evidence now supports the idea that particle count matters more than cholesterol weight.
A 2024 consensus statement in the Journal of Clinical Lipidology from the National Lipid Association reviewed the available scientific evidence and concluded that ApoB is superior to standard LDL cholesterol (LDL-C) for assessing cardiovascular risk. The experts noted that ApoB accurately reflects the total burden of plaque-causing particles.
This becomes especially important when a patient experiences discordance (dis-KORD-uhns). Discordance happens when two related medical tests give conflicting results. For example, a person might have a “normal” LDL-C weight, but a dangerously high ApoB particle count.
When these numbers disagree, which one predicts the actual risk of a heart attack?
A 2025 review in Atherosclerosis looked specifically at this discordance. The researchers found that when LDL-C and ApoB disagree, a person’s actual risk of cardiovascular disease follows the ApoB number. If your LDL is low but your ApoB is high, your risk is high.
Genetic studies strongly support this. A 2019 study in Circulation: Genomic and Precision Medicine analyzed genetic data from over 57,000 people. Researchers found that individuals who carried rare genetic variants that naturally lowered their ApoB levels had a 72% lower risk of coronary heart disease compared to non-carriers.
Beyond the Heart: Stroke and Brain Health
The benefits of keeping ApoB low extend beyond the heart and into the brain.
A 2022 study in the Annals of Neurology followed over 104,000 individuals to see which cholesterol markers best predicted ischemic stroke (strokes caused by blood clots). The researchers found that the proportion of strokes attributable to elevated ApoB was double the proportion attributable to elevated LDL-C.
Furthermore, a 2023 study in Atherosclerosis looked at patients who had already experienced a stroke. The researchers found that ApoB levels were consistently associated with narrowing in the brain’s arteries, even in patients who were actively taking statin medications to lower their cholesterol. Standard LDL-C did not show this same consistent link in statin-treated patients.
There is also early research exploring how these particles affect cognitive decline. A 2019 study in JAMA Neurology found an association between elevated LDL cholesterol, rare genetic variants of the APOB gene, and early-onset Alzheimer’s disease. While more research is needed to understand this connection, it suggests that managing plaque-causing particles may be important for long-term brain health.
The Role of Remnant Cholesterol and Small Dense LDL
While ApoB gives a total count of all dangerous particles, scientists are also discovering that certain types of particles within that total count carry their own specific risks.
Standard lipid panels calculate LDL, but they often miss “remnant cholesterol” (cholesterol carried by other plaque-causing particles like VLDL). A 2024 study in Arteriosclerosis, Thrombosis, and Vascular Biology found that peripheral artery disease (PAD) risk is driven more by these remnant cholesterol particles than by standard LDL.
Similarly, a 2025 study in the same journal evaluated “small, dense LDL” particles. The researchers found that estimating the amount of small, dense LDL was highly predictive of cardiovascular events, sometimes even more so than total ApoB.
What does this mean for the average person? It reinforces why ApoB might be the most accurate heart health test you have never had. Because ApoB counts all of these particles (including remnants and small dense LDL), it provides a comprehensive snapshot of your risk in a single test.
Who Benefits Most From ApoB Testing?
While anyone can ask their doctor for an ApoB test, research shows it is particularly useful for certain groups of people where standard LDL tests often fail to tell the whole story.
According to the 2024 National Lipid Association consensus, ApoB testing is highly recommended for individuals with:
- High triglycerides: High triglycerides often alter the size of cholesterol particles, making standard LDL calculations inaccurate.
- Type 2 Diabetes or Insulin Resistance: These conditions often cause the body to produce many small, dense cholesterol particles. A patient might have a “healthy” LDL weight but a dangerously high particle count.
- Metabolic Syndrome and Obesity: Similar to diabetes, these conditions alter understanding fat metabolism: how your body actually stores and burns fat, leading to misleading standard cholesterol results.
- Very low LDL-C on medication: If you are taking a statin and your LDL is very low, an ApoB test can verify if your particle count is actually low, or if residual risk remains.
Common Questions About ApoB Testing
Is ApoB an experimental or unproven test?
No. A 2023 review in the Journal of the American Heart Association clearly states that ApoB is a highly standardized, accurate, and inexpensive test. Multiple international expert groups have declared it ready for routine clinical care.
Do I need to fast for an ApoB test?
No. Unlike standard cholesterol panels that can be heavily skewed by a recent meal (especially the triglyceride portion), ApoB levels remain very stable whether you have eaten recently or not.
If ApoB is better, why do doctors still use LDL?
Standard lipid panels have been used for decades. All major historical clinical trials based their treatment guidelines on LDL-C. Transitioning the entire medical system to a new standard takes time. However, a 2026 computer simulation study in JAMA found that using ApoB goals to guide preventative treatment is highly cost-effective and produces more healthy life-years than using standard LDL goals.
The Bottom Line / Takeaways
- Particle count matters: ApoB measures the exact number of plaque-causing particles in your blood, whereas standard LDL measures the total weight of the cholesterol inside them.
- ApoB is often more accurate: When LDL and ApoB numbers disagree, your actual risk of heart disease and stroke follows the ApoB number.
- It is crucial for metabolic issues: If you have diabetes, high triglycerides, or obesity, standard LDL tests may underestimate your risk, making ApoB testing highly valuable.
- It is accessible: ApoB is a standardized, relatively inexpensive blood test that does not require fasting.
- Standard tests still have value: You do not need to throw away your standard lipid panel. ApoB is best used alongside traditional tests to give your doctor a complete picture of your cardiovascular health.
Quick Reference: Key Studies
| Study Focus | Key Finding | Source |
|---|---|---|
| Clinical Consensus | ApoB is superior to LDL-C in risk assessment; testing is accurate and underutilized. | PMID 39256087 |
| Stroke Risk | Proportion of ischemic strokes attributable to elevated ApoB is double that of LDL-C. | PMID 35635038 |
| Genetic Risk | Rare genetic variants that lower ApoB are associated with a 72% reduced risk of coronary heart disease. | PMID 30939045 |
| Cost-Effectiveness | Using ApoB to guide preventative treatment is highly cost-effective compared to LDL-C. | PMID 41949879 |
| Test Standardization | ApoB is a highly standardized test, often more precise than calculated LDL-C. | PMID 37489721 |
| Brain Arteries | ApoB is consistently associated with intracranial artery narrowing, even in statin users. | PMID 36966561 |
Last updated: June 2026
This article synthesizes findings from peer-reviewed research. It is for educational purposes only and does not constitute medical advice. Consult a healthcare provider before starting any new regimen.
Leave a Reply